

Summary
Non-Celiac Gluten Sensitivity (NCGS) is a relatively new disorder that is associated with the consumption of wheat and other gluten-containing foods. Its mechanism is not yet fully elucidated, and without proper evaluation it can be confused with celiac disease, wheat allergies, or other gastrointestinal problems. This article discusses the clinical and pathophysiologic features and diagnostic approach for individuals with possible NCGS.
- Nutrition Physiology
- Nutrition
- Nutrition Physiology
Non-Celiac Gluten Sensitivity (NCGS) is a relatively new disorder that is associated with the consumption of wheat and other gluten-containing foods. Its mechanism is not yet fully elucidated, and without proper evaluation it can be confused with celiac disease (CD), wheat allergies, or other gastrointestinal problems. Douglas L. Seidner, MD, Vanderbilt University Medical Center, Nashville, Tennessee, USA, discussed the clinical and pathophysiologic features and diagnostic approach for individuals with possible NCGS.
Patients with NCGS present with a wide array of gastrointestinal and extra-intestinal symptoms. About 0.63% to 6% of the population report having NCGS. Diagnosis is based on the rapid occurrence and subsidence of symptoms with the ingestion and withdrawal of gluten, negative CD serology, and normal duodenal histology while on a diet that contains gluten, negative immunoglobulin E-based tests for wheat allergy, and positive symptom response to a controlled gluten challenge [Volta U et al. Cell Mol Immunol 2013]. Since NCGS is a “diagnosis of exclusion”, its existence has been somewhat controversial.
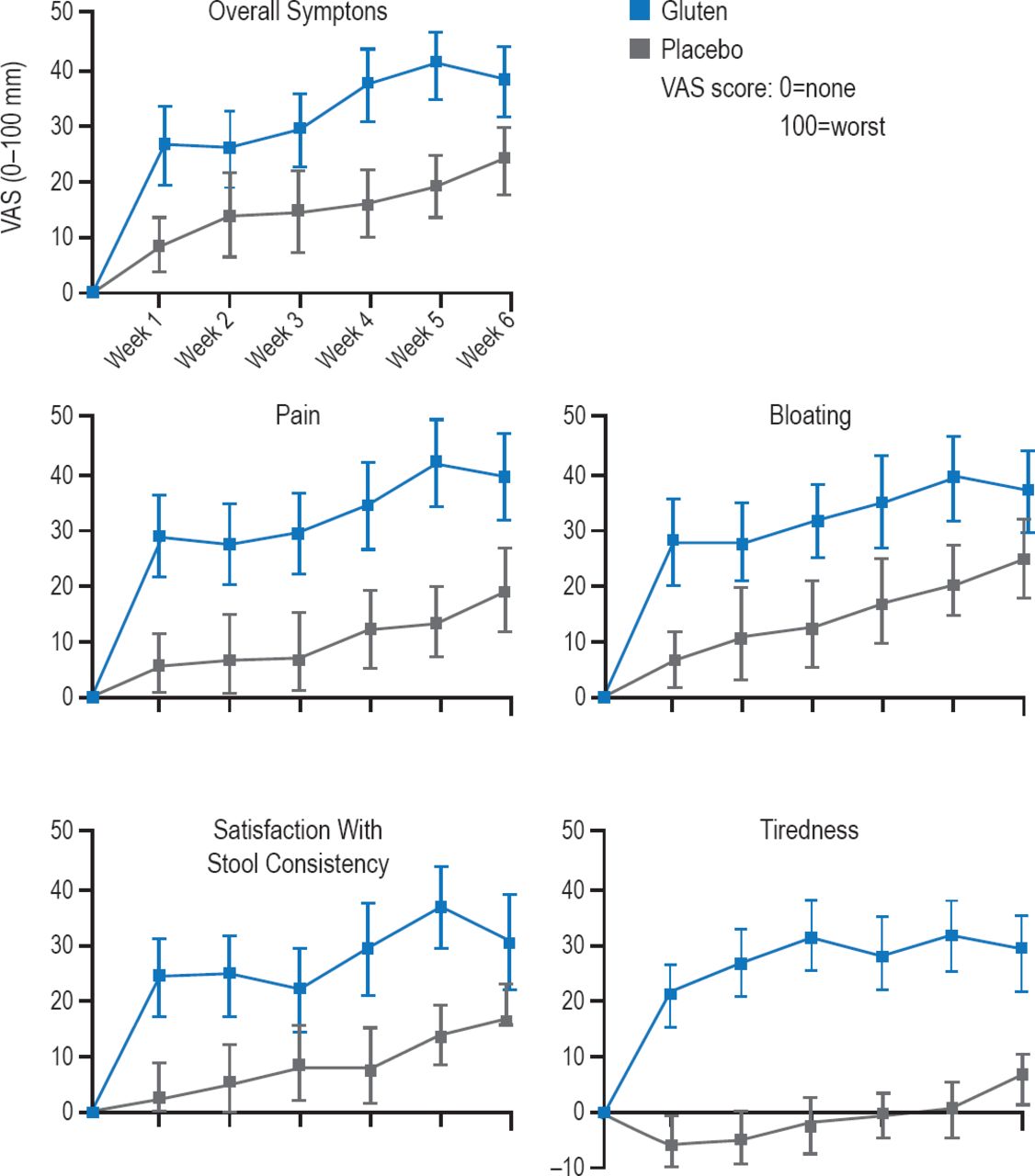
Dr. Seidner reviewed several controlled trials that evaluated the relationship between gluten and gastrointestinal symptoms in NCGS individuals. One of these was a double-blind, randomized, placebo-controlled rechallenge trial in subjects with irritable bowel syndrome (IBS)-like symptoms in whom CD was excluded and who were improved on a gluten-free diet. Participants received either a gluten or placebo supplemented gluten-free diet for 6 weeks. Significantly more participants in the gluten group reported that their symptoms were inadequately controlled compared with those receiving placebo (p=0.0001). Within 1 week of gluten exposure, subjects had significantly worse overall symptoms (p=0.047), pain (p=0.016), bloating (p=0.031), satisfaction with stool consistency (p=0.024), and tiredness (p=0.001) as shown in Figure 1 [Biesiekierski JR et al. Am J Gastroenterol 2011]. Though numerous potential biomarkers were measured in this study, the mechanism of NCGS could not be identified.

Symptom Changes While on Gluten and Placebo Diets
Reproduced from Biesiekierski JR et al. Gluten causes gastrointestinal symptoms in subjects without celiac disease: a double-blind randomized placebo-controlled trial. Am J Gastroenterol 2011;106(3):508–514. With permission from the Nature Publishing Group.
The second study was a chart review including patients with an IBS-like presentation who had been diagnosed with wheat sensitivity (WS; n=276). One hundred CD patients and 50 IBS patients served as controls. The main histologic characteristic of WS patients was eosinophil infiltration of the duodenal and colon mucosa. Two groups of WS patients were identified: those with WS alone and those with WS and multiple food hypersensitivity. The investigators concluded that non-celiac WS is a distinct condition with two distinct populations: those with characteristics similar to those found in CD patients (WS alone) and those with characteristics more similar to allergic patients (WS plus multiple food sensitivity) [Carroccio A et al. Am J Gastroenterol 2012].
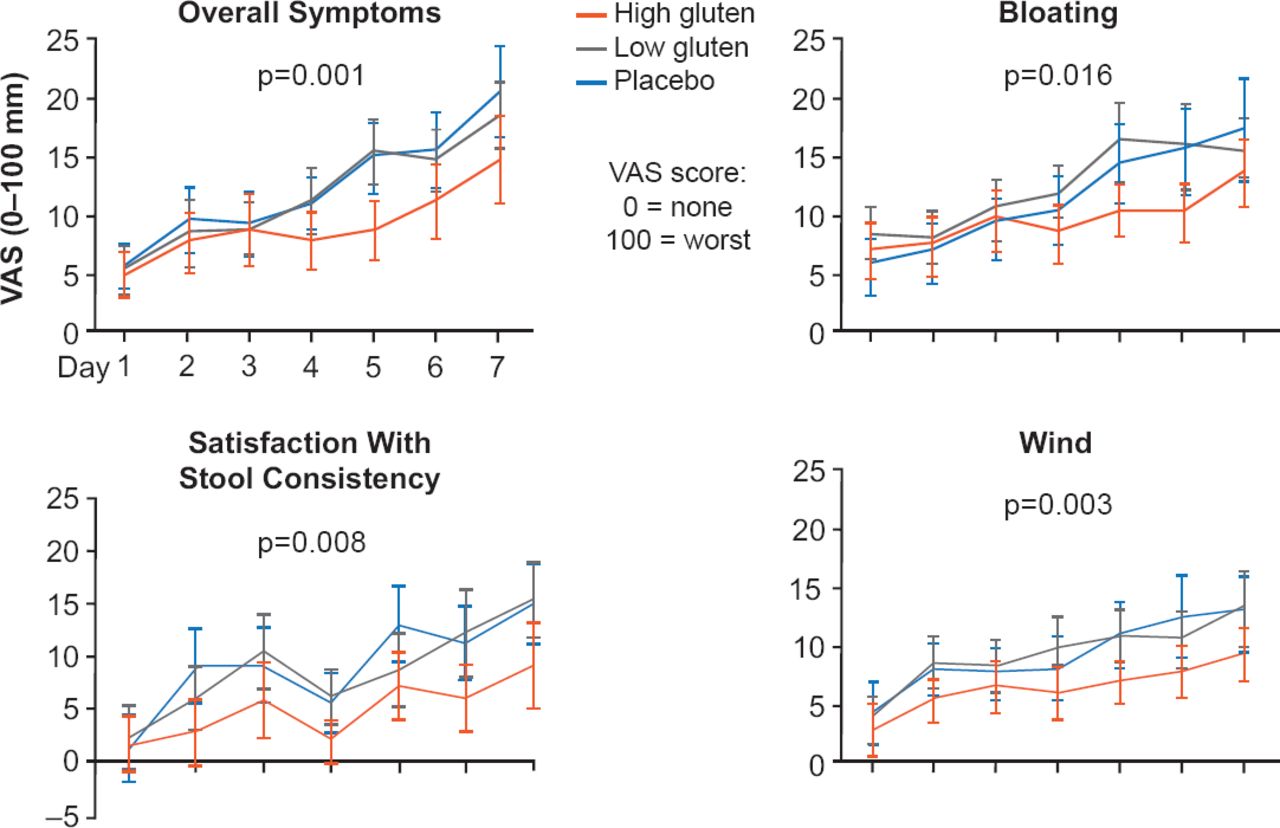
The third study was a randomized double-blind crossover trial of 37 subjects with NCGS and IBS-like symptoms. Subjects were placed on a 2-week diet of reduced FODMAPs (fermentable, oligo-, di-, monosaccharides, and polyols) followed by a high-gluten (16 g/day), low-gluten (2 g/day and 14 g whey protein/day), or control FODMAPs diet (16 g whey protein/day) for 1 week. Subjects were exposed to all three diets in a random fashion with a 2-week FODMAPs only washout period. Gastrointestinal symptom severity significantly (p<0.0001) improved during reduced FODMAP intake but worsened on diets that included gluten or whey protein (Figure 2). Gluten-specific effects were observed in 8% of participants. The authors concluded that a gluten-free diet does not improve symptoms in NCGS [Biesiekierski JR et al. Gastroenterology 2013].

Symptom Severity During 7-Day Study Phase Compared With Run-in Phase
NS=nonsignificant; VAS=visual analog scale.
Reproduced from Biesiekierski JR et al. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology 2013;145(2):320–328. With permission from Elsevier.
Taken together, these three studies do not fully resolve the controversy over the presence of NCGS. Because NCGS and CD have many symptoms that are similar it is recommended that clinical guidelines be used to help manage individuals with these conditions. Below are some of the guideline recommendations recently made by the America College of Gastroenterology [Rubio-Tapia A et al. Am J Gastroenterol 2013].
-
A diagnosis of NCGS should not rely on symptom response to gluten-free diet alone and should be considered only after CD has been excluded with appropriate testing.
-
Standard diagnostic tests should not be relied upon to exclude CD in patients already adhering to a gluten-free diet.
-
CD should be differentiated from NCGS in order to identify the risk for nutritional deficiency states, complications of CD, risk for CD and associated disorders in family members, and to influence the degree and duration of adherence to the gluten-free diet.
-
HLA-DQ2/DQ8 genotyping should be used to try to exclude CD prior to embarking on a formal gluten challenge.
-
Formal gluten challenge should be considered, where necessary, to diagnose or exclude CD in patients already adhering to a gluten-free diet.

The editors would like to thank the many members of the American Society for Nutrition presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.