

Summary
Shorter overall treatment time with radiotherapy (RT) appears to improve outcomes in patients with non—small cell lung cancer (NSCLC) compared with longer overall treatment time. This article outlines optimal RT dose and fractionation for concurrent and sequential schedules for stage III NSCLC.
- Respiratory Cancers
- Radiology
- Radiation Therapy
- Cancer
- Respiratory Cancers
- Radiology
- Radiation Therapy
- Oncology
- Cancer
Shorter overall treatment time with radiotherapy (RT) appears to improve outcomes in patients with non-small cell lung cancer (NSCLC) compared with longer overall treatment time. Dirk De Ruysscher, MD, PhD, Leuven Cancer Institute, Leuven, Belgium, outlined optimal RT dose and fractionation for concurrent and sequential schedules for stage III NSCLC.
The dosage and timing of RT affect the local control of NSCLC. For example, when RT is not administered during chemotherapy (CT), longer progression-free survival is achieved with RT that is given for a shorter period of time (<4 weeks) compared with a longer period of time (5 weeks) [Fowler JF et al. Int J Radiat Oncol Biol Phys 2004]. A meta-analysis demonstrated that better overall survival is achieved in patients with stages I through III NSCLC when sequential RT is given for a shorter period of time [Mauguen A et al. J Clin Oncol 2012].
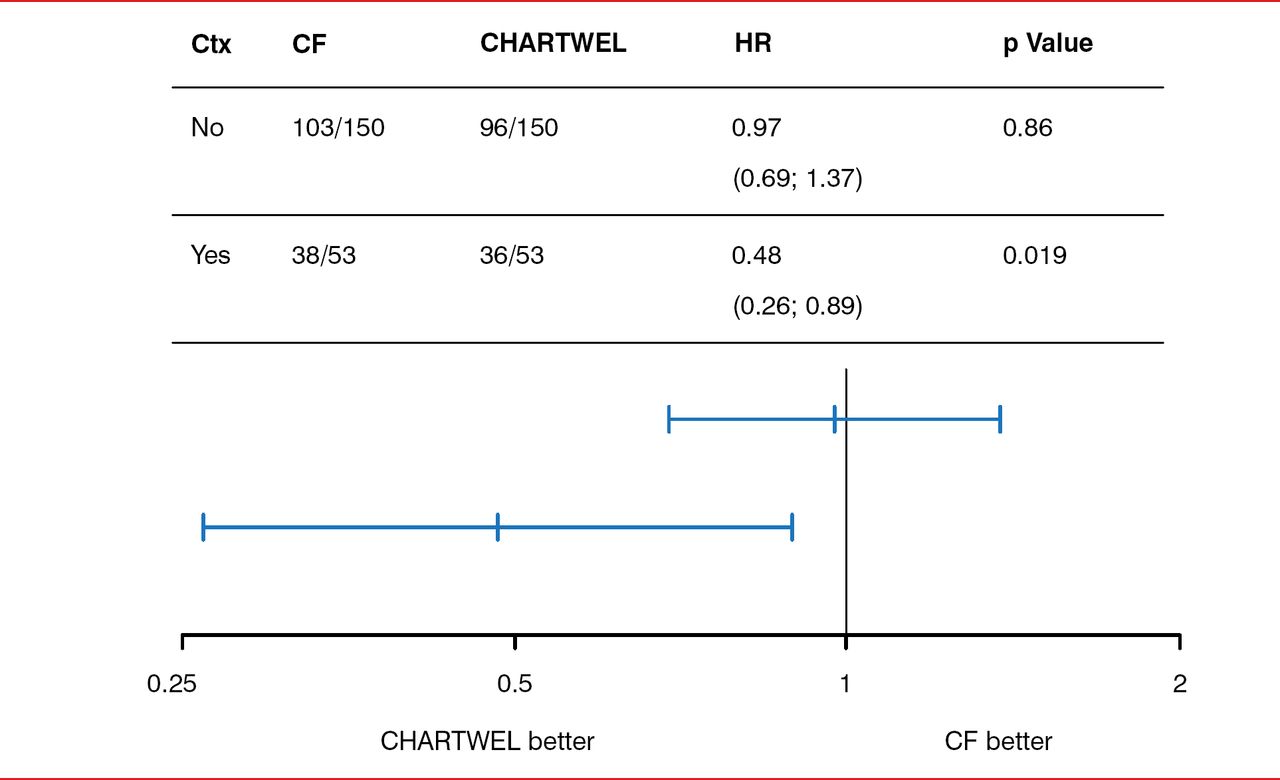
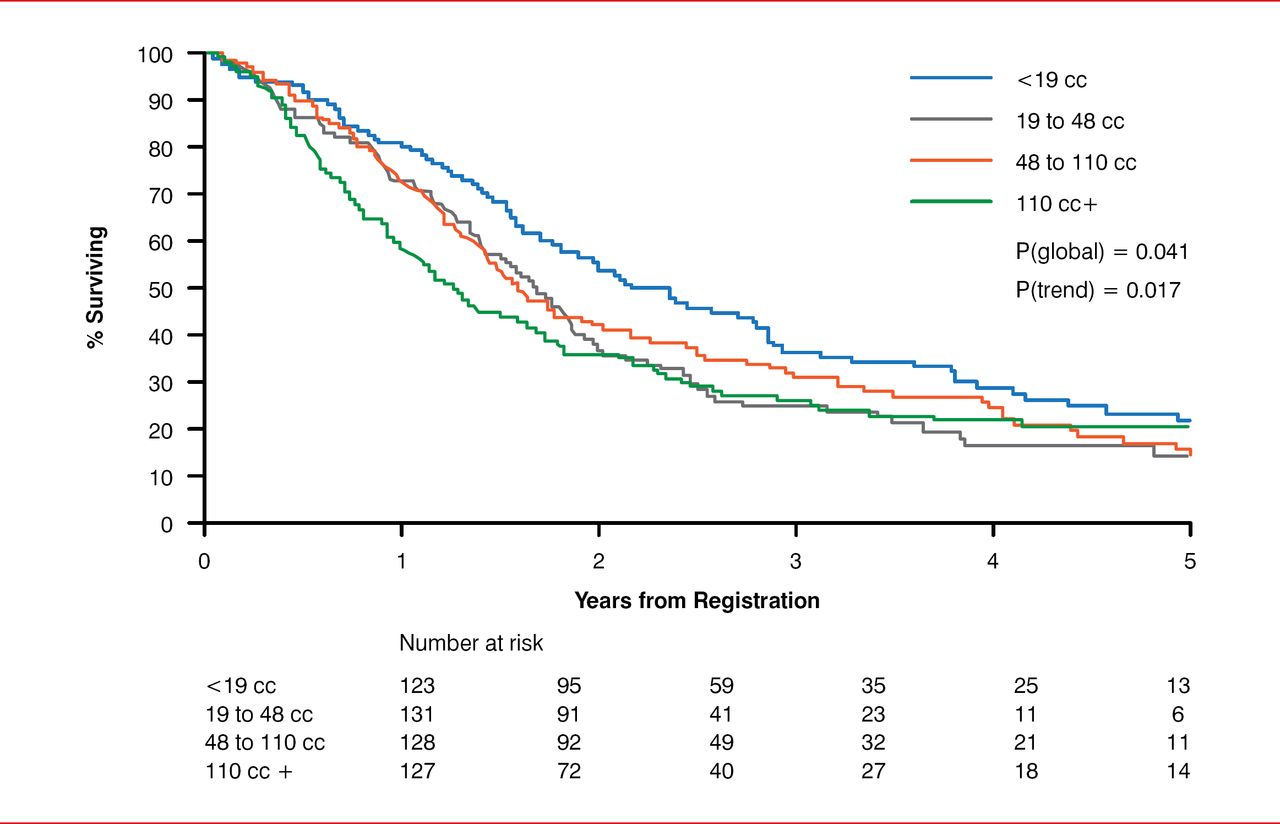
The dosage and timing of RT are also important in induction CT. Dr. De Ruysscher suggested that long-term survival can be achieved even in patients with large tumor volumes when accelerated RT is administered. In the CHART Weekend Less (CHARTWEL) trial, conventional fractionation that consisted of 66 Gy in 33 fractions for 6.6 weeks was compared with an accelerated, or CHARTWEL, regimen that consisted of 60 Gy in 40 fractions for 2.5 weeks [Baumann M et al. Radiother Oncol 2011]. The CHARTWEL regimen resulted in improved outcomes compared with conventional fractionation (Figure 1). However, although greater tumor volume is associated with greater local failure when conventional fractionation is given, this appears to not be the case with accelerated fractionation (the CHARTWEL regimen). Similarly, in the Trans-Tasman Radiation Oncology Group 99.05 trial, tumor volume was not associated with survival at 4 years in patients who received 50 Gy in 20 fractions, despite initial differences in survival (Figure 2) [Ball DL et al. Radiother Oncol 2013].

Effect of Radiotherapy Dose and Timing on Outcomes of Induction Chemotherapy in NSCLC
CF=controlled fractionation; CHARTWEL= CHART Weekend Less; Ctx=chemotherapy; NSCLC=non-small cell lung cancer.
Reproduced from Baumann M et al. Final results of the randomized phase III CHARTWEL-trial (ARO 97-1) comparing hyperfractionated-accelerated versus conventionally fractionated radiotherapy in non-small cell lung cancer (NSCLC). Radiother Oncol. 2011;100(1):76–85. With permission from Elsevier.

Effect of Tumor Volume on Survival With Accelerated Radiotherapy
Reproduced from Ball DR et al. The complex relationship between lung tumor volume and survival in patients with non-small cell lung cancer treated by definitive radiotherapy: a prospective, observational prognostic factor study of the Trans-Tasman Radiation Oncology Group (TROG 99.05). Radiother Oncol. 2013;106(3):305–311. With permission from Elsevier.
Concurrent CT and RT are considered better than sequential CT and RT, according to level I evidence. A meta-analysis demonstrated that concurrent CT and RT results in better outcomes compared with sequential therapy across many trials [Auperin A et al. J Clin Oncol 2010]. A Phase 3 trial compared 60 to 66 Gy in 2 Gy/d fractions for 6 to 7 weeks with 66 Gy in 24 fractions for >5 weeks, both of which were concurrent with CT (cisplatin and etoposide, cisplatin and vinorelbine, or cisplatin alone). All of these regimens had similar efficacy. Dr. De Ruysscher suggested that in the future, clinical trials should compare concurrent CT and RT with sequential RT given at a higher biologic dose.
In concurrent chemoradiotherapy, the dose of radiation given is important. It is generally thought that the higher the dose of radiation, the better the efficacy. However, Dr. De Ruysscher highlighted the surprising findings of a trial that compared 60 Gy for 6 weeks with 74 Gy for 7.5 weeks. Interestingly, at 18-month follow-up, the survival rate and median overall survival were 53.9% and 19.5 months, respectively, in patients who received 74 Gy and 66.9% and 28.7 months, respectively, in patients who received 60 Gy (p=0.0007). In addition, the 74-Gy dose resulted in a significantly greater local progression rate (p=0.0319) and trended toward worse distant failure (p=0.1576) compared with the 60-Gy dose. An ongoing trial will provide further information regarding the effect of the dose of RT with concurrent CT (NCT1486602). This open-label, dose-escalation, Phase 1 trial of patients with NSCLC will evaluate paclitaxel and carboplatin plus hypofractionated RT, or paclitaxel plus carboplatin after RT is completed. The primary outcome is the maximum tolerable RT dose fraction in the concurrent arm.
Dr. De Ruysscher concluded by stating that in his opinion, the most optimal nonconcurrent RT at this time is using an accelerated schedule. For concurrent chemoradiotherapy, the standard regimen should be retained at this point, as decreasing the overall treatment time with RT has not yet been demonstrated to improve outcomes.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.