

Summary
A meta-analysis of 6 randomized trials demonstrated that when compared with aspirin therapy alone, dual antiplatelet therapy beyond 1 year decreased the risk of major adverse cardiovascular events, myocardial infarction, stroke, and cardiovascular death among high-risk patients with previous myocardial infarction while increasing the risk of major bleeding.
- DAPT
- dual antiplatelet therapy
- MACE
- major adverse cardiovascular event
- major bleeding
- MI
- myocardial infarction
A meta-analysis of randomized controlled trials has demonstrated a substantial reduction in cardiovascular (CV) outcomes, including CV mortality, with dual antiplatelet therapy (DAPT) continued beyond 1 year vs aspirin alone, among patients with a prior myocardial infarction (MI) [Udell JA et al. Eur Heart J. 2015].
The recent trials examining the effect of extended DAPT in a variety of patient populations have produced heterogeneous results regarding its safety and efficacy, according to Jacob A. Udell, MD, MPH, University of Toronto, Toronto, Canada. He noted that in clinical practice DAPT is stopped at 1 year in about 50% of patients because of the lack of long-term data.
Dr Udell and colleagues conducted a systematic review and meta-analysis that evaluated whether long-term DAPT reduced CV risk when compared with aspirin alone in patients with a history of prior MI. The primary end point was a composite of major adverse CV events (MACEs) defined as CV death, MI, and stroke. The secondary end points included CV death, MI, stroke, non-CV death, all-cause mortality, major bleeding, and stent thrombosis.
The key features of the 6 trials included in the meta-analysis are shown in Table 1. The mean follow-up was 30 months, and there was a total of 2273 MACEs. The mean age of the patients was 64 years; 24% were women; and the mean time from MI was 18 months. Notably, few patients had unstable angina (7%), prior stroke or transient ischemic attack (3%), or prior coronary bypass surgery (7%).
Trials Evaluated in Meta-analysis
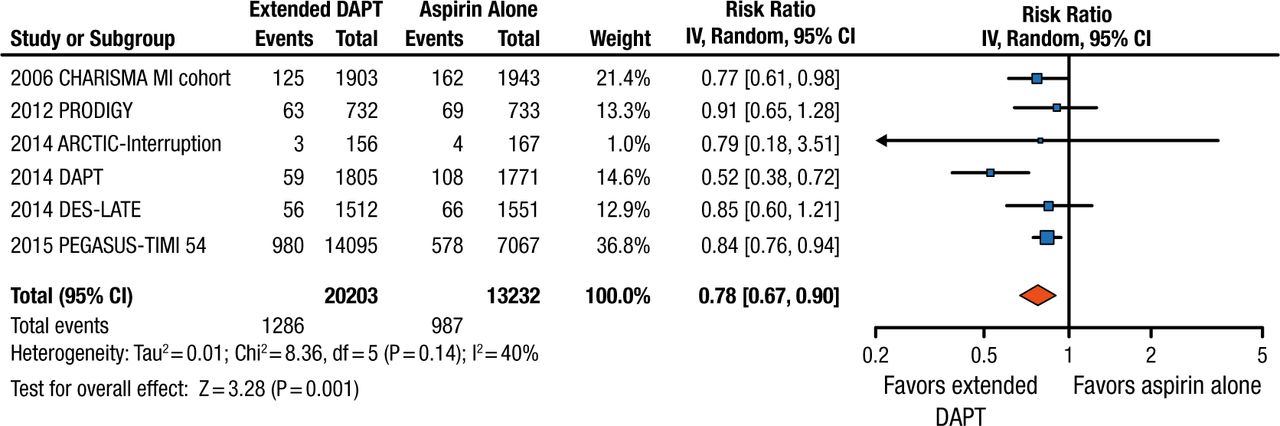
The results for the primary end point showed a significant risk reduction of 22% with prolonged DAPT, with low heterogeneity across the trials. The rate of MACEs was 6.4% among the 20 203 patients assigned to DAPT vs 7.5% among the 13 232 patients receiving aspirin alone (RR, 0.78; P = .001; Figure 1). The rate of CV death alone was 2.3% for patients on DAPT vs 2.6% of those receiving aspirin (RR, 0.85; 95% CI, 0.74 to 0.98; P = .03). Prolonged DAPT also significantly reduced the risk of individual CV end points, such as MI (RR, 0.70; P = .003), stroke (RR, 0.81; P = .02), and stent thrombosis (RR, 0.50; P = .02).

Primary End Point: Major Adverse Cardiovascular Event
Risk of major adverse cardiovascular events comparing extended dual antiplatelet therapy vs. aspirin alone. Square data markers represent risk ratios and horizontal lines the 95% confidence intervals with marker size reflecting the statistical weight of the study using inverse variance random effects meta-analysis. A diamond data marker represents the overall risk ratios and 95% confidence intervals for major adverse cardiovascular events. There was no significant between-trial heterogeneity (Q statistic = 8.36, d.f. = 5; P = 0.14; I2 = 40%).
CV, cardiovascular; DAPT, dual antiplatelet therapy; MI, myocardial infarction.
Reprinted from Udell JA et al, Long-term dual antiplatelet therapy for secondary prevention of cardiovascular events in the subgroup of patients with previous myocardial infarction: a collaborative meta-analysis of randomized trials, Eur Heart J, 2015, by permission of Oxford University Press.
The rate of major bleeding was significantly higher among patients receiving DAPT vs aspirin alone, at 1.9% vs 1.1%, respectively (RR, 1.73; P = .004). However, the rate of other bleeding events, such as intracranial hemorrhage (ICH), fatal bleeding, non-CV death, and all-cause death, was not significantly different between the treatment groups. All subgroup analyses demonstrated that extended DAPT was more effective than aspirin alone regardless of age, sex, DAPT regimen, index acute coronary syndrome, time from index MI, and history of percutaneous coronary intervention.
Dr Udell concluded that extending DAPT beyond 1 year decreased the risk of MACE, MI, stroke, and CV death among high-risk patients with previous MI when compared with aspirin therapy alone. It also increased the risk of major bleeding but not fatal bleeding or ICH, and it did not increase the risk of death due to non-CV causes. However, he cautioned that prolonged DAPT is not appropriate for patients with anticoagulation issues, recent bleeding events or surgery, or history of ICH and that very few patients studied had prior stroke or a transient ischemic attack.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.