

Summary
Newer syncope protocols can improve diagnostic accuracy and risk stratification in patients presenting with syncope, leading to more appropriate treatment and reduced recurrence rates and mortality. Adherence to syncope protocols also reduces hospital admissions, inappropriate testing, and costs of diagnosis and treatment.
- cardiac syncope
- carotid sinus massage
- cost-effectiveness
- diagnosis
- electrocardiography
- epilepsy
- insertable loop recorder
- pacemaker
- psychogenic pseudosyncope
- protocol
- sudden cardiac death
- syncope
- tilt testing
- interventional techniques & devices
- cardiology & cardiovascular medicine clinical trials
Causes of transient loss of consciousness include trauma, syncope, seizures, intoxications, and metabolic disturbances. False transient loss of consciousness can occur due to psychogenic causes, pseudosyncope or pseudoseizure, “drop attacks,” or cataplexy. True syncope can be due to neurally mediated reflex, orthostatic hypotension, cardiac arrhythmia, structural cardiopulmonary conditions, or unexplained causes.
The Signature Group developed an algorithm for rapid prediction of syncope onset by analyzing heart rate and blood pressure in 1155 patients with previous syncope [Virag N et al. Heart Rhythm. 2007]. In this study, electroencephalogram video studies showed that heart rate parameters changed in different ways during episodes of syncope, epilepsy, and psychogenic pseudosyncope. The objective of the study was to find a quicker, less expensive way to diagnose syncope. To accomplish this, the researchers recorded electrocardiograms (ECGs) of patients during electroencephalogram video monitoring with the hypothesis that if the type of syncope could be identified using ambulatory ECG, the same principles could be applied to medium-term external or long-term implantable loop recorders (ILRs). Dr Richard Sutton, DSc, MBBS, Imperial College, London, United Kingdom, presented results. Among 45 patients, syncope was diagnosed as epilepsy (n = 17), psychogenic pseudosyncope (n = 8), or vasovagal syncope (n = 20) on the basis of a measure called marginality, a new approach to imaging in syncope diagnosis methods. The study results are summarized in Table 1, showing that marginality was low (< 4%) for tachycardia and reflex syncope but higher (> 10%) for focal epilepsy and nonepileptic attack disorder.
Details of Syncope Diagnoses Made by Electrocardiogram Marginality
David G. Benditt, MD, University of Minnesota, Minneapolis, Minnesota, USA, discussed assessing risk in patients presenting with syncope, and he indicated that patients with syncope may be at increased risk of mortality, including sudden cardiac death. Other risks include serious injury and loss of independence in elderly patients. There is no universal consensus on how to assess risk, but several studies are ongoing. Studies of major syncope risk stratification systems are summarized in Table 2.
Major Syncope Risk Stratification Systems
The EGSYS study had the most robust data and employed a point score that is useful in the clinic, according to Dr Benditt. The EGSYS 2 follow-up data demonstrated an approximately 20% syncope recurrence rate at 2 years, regardless of the underlying cause [Ungar A et al. Eur Heart J. 2010]. Predictors of mortality included age (P < .0001), trauma (P = .018), heart disease or abnormal ECG (P < .0001), male sex (P = .030), and hypertension (P = .002). An international meta-analysis including 43 315 patients from 11 studies identified high-risk markers of adverse outcomes, including palpitations preceding syncope, heart disease, and syncope during effort [D’Ascenzo F et al. Int J Cardiol. 2013].
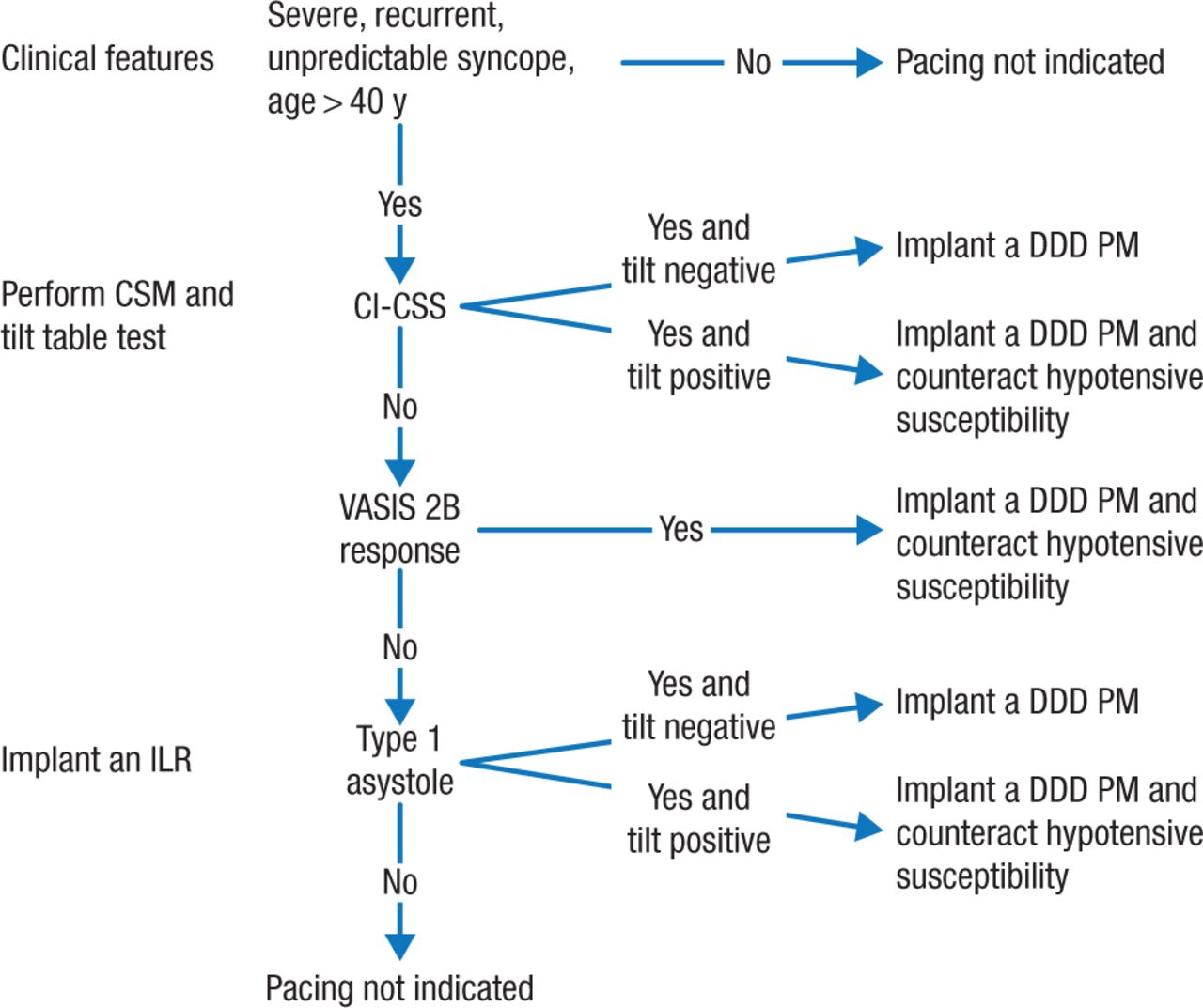
The risks associated with syncope might be reduced with cardiac pacing in appropriate cases. Michele Brignole, MD, Ospedali del Tigullio, Lavagna, Italy, studied the benefits of cardiac pacing for patients with reflex syncope. The SUP2 study [Brignole M et al. Eur Heart J. 2015] evaluated 253 patients with severe unpredictable recurrent reflex syncope with carotid sinus massage (CSM), tilt testing (TT) if CSM was negative, and ILR if TT was negative. Patients with an asystolic response to 1 of the tests received a dual-chamber pacemaker (n = 120). The recurrence rate among these patients was 9% at 1 year and 15% at 2 years, compared with 22% at 1 year and 37% at 2 years among patients with an ILR and no pacemaker (P = .004).
The prevalence of carotid sinus syndrome was 2 to 5 times higher than in the general syncope population. Syncope was more likely to recur in patients with mixed forms of carotid sinus syndrome or positive mixed or vasodepressor TT. A positive TT might indicate hypotensive susceptibility, which can cause syncope recurrence regardless of the etiology and mechanism of syncope [Solari D et al. Europace. 2014; Sutton R, Brignole M. Eur Heart J. 2014].
The algorithm used to identify patients for pacemaker implantation in the SUP2 study was revised on the basis of evidence from this and other studies (Figure 1).

Decision Tree: Pacing for Neurally Mediated Syncope
CI-CSS, cardioinhibitory carotid sinus syndrome; CSM, carotid sinus massage; DDD PM, dual-chamber pacemaker; ILR, implantable loop recorder; VASIS 2B, Vasovagal Syncope International Study 2B.
Reproduced with permission from M Brignole, MD.
Standardization of syncope management through the introduction of syncope protocols such as this decision tree can help reduce the number of admissions, tests performed, and rate of unexplained syncope. Mohamed H. Hamdan, MD, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, USA, discussed how syncope protocols and clinics can improve the cost-effectiveness of syncope management.
The cost of syncope management is determined by hospital admissions, test utilization, and the rates of unexplained syncope and misdiagnosis. According to the European Society of Cardiology guidelines, high-risk criteria requiring prompt hospitalization or intensive evaluation are as follows: severe structural heart disease, clinical or ECG features suggesting arrhythmic syncope, and important comorbidities [Moya A et al. Eur Heart J. 2009]. A comparison of standardized admission criteria (Faint-Algorithm) with clinical practice found that in a single center, 58% of admissions and 6% of discharges were inappropriate [Daccarett M et al. Europace. 2011]. Other data demonstrated high rates of inappropriate testing among patients presenting with syncope [Edvardsson N et al. Europace. 2011; Mendu ML et al. Arch Intern Med. 2009; Pires LA et al. Arch Intern Med. 2001]. Studies have demonstrated rates of unexplained syncope of 52% [Brignole M et al. Pacing Clin Electrophysiol. 2011] and misdiagnoses of 12.9% [Josephson CB et al. Can J Neurol Sci. 2007] and 39% [MacCormick JM et al. Ann Emerg Med. 2009].
Several studies have shown that establishing syncope protocols and units can improve diagnosis, reduce hospitalizations, and lower costs (Table 3).
Studies Comparing Syncope Protocols and Unit Care vs Conventional Diagnosis and Care
The evidence shows that differential diagnosis between epilepsy and syncope may be difficult, especially in retrospect. Cardiovascular evaluation including CSM, TT, and ILR may identify an alternative diagnosis in many patients with apparent epilepsy.
Appropriate use of syncope protocols and syncope units can increase the rate of appropriate diagnoses and decrease admission rates, hospital stays, and unnecessary testing. The University of Wisconsin established a Faint and Fall Clinic that provides better care while being profitable. Despite the decrease in admissions and tests per diagnosis, hospitals could have increased margins due to improved quality of care and associated increase in market share.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.