

Summary
For patients with rheumatoid arthritis (RA) who fail methotrexate (MTX), using a biologic instead of triple therapy first is not a cost-effective use of health care resources due to the large additional costs for very small benefits. This article presents the results of a randomized noninferiority trial that compared the cost-effectiveness of treating patients who fail MTX with a biologic first or adding triple therapy followed by a biologic.
- Rheumatology Clinical Trials Rheumatoid Arthritis
- Rheumatology Clinical Trials
- Rheumatology
- Rheumatoid Arthritis
For patients with rheumatoid arthritis (RA) who fail methotrexate (MTX), using a biologic instead of triple therapy first is not a cost-effective use of health care resources due to the large additional costs for very small benefits.
Nick Bansback, PhD, University of British Columbia, Vancouver, British Columbia, Canada, presented the results of a randomized noninferiority trial that compared the cost-effectiveness of treating patients who fail MTX with a biologic first or adding triple therapy followed by a biologic.
The analysis was based on the Rheumatoid Arthritis: Comparison of Active Therapies in Patients With Active Disease Despite Methotrexate Therapy study [RACAT; O'Dell JR et al. N Engl J Med. 2013], a 48-week double-blind noninferiority trial that randomized 353 patients with active RA despite MTX therapy to either a triple regimen of disease-modifying antirheumatic drugs (MTX, sulfasalazine, and hydroxychloroquine) or etanercept (ETN) plus MTX. The trial showed that triple therapy was noninferior to ETN plus MTX in these patients.
In the current study, Bansback and colleagues first conducted a within-trial incremental cost-effectiveness ratio (ICER) analysis that considered all the incremental costs between the 2 strategies, including drugs, visits, tests, surgical procedures, other hospitalizations, and work absences, as well as the benefits in terms of quality-adjusted life years (QALYs). This ratio indicated the value for money of an intervention.
Based on the assumption that we do not pay > $100 000.00 for an additional QALY in the current health care system, the study considered any number below that of reasonable value.
The results of this analysis at 24 weeks showed that the cost of ETN plus MTX was substantially higher than triple therapy, largely because of the higher cost of ETN. The ICER at 24 weeks for ETN was $2.67 million per QALY, substantially higher than the $100 000.00 cutoff benchmark (Figure 1).

Within-Trial Analysis at 24 Weeks: ICER for Etanercept
ICER, incremental cost-effectiveness ratio; M, million; QALY, quality-adjusted life year.
Reproduced with permission from N Bansback, PhD.
In a second analysis at 48 weeks, the ICER was $0.98 million per QALY for the ETN strategy, which was also found not to be very cost-effective.
Using a lifetime model based on a previous analysis to examine the cost-effectiveness of these 2 strategies over the longer term, the study also found that the strategy of using ETN was not cost-effective even when considering the potential impact of changes in radiographic progression [Finckh A et al. Ann Intern Med. 2009].
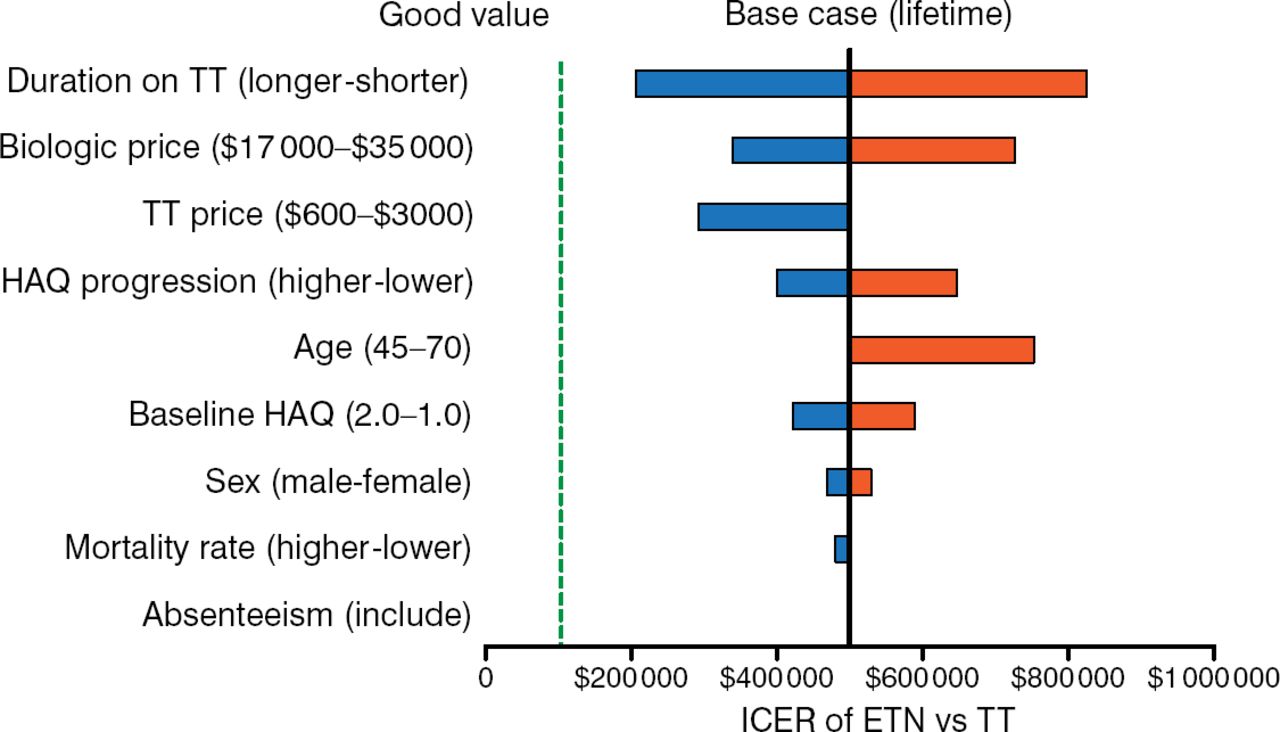
A sensitivity analysis provided data as well to provide confidence that using ETN first would not be cost-effective, said Dr Bansback. As shown in Figure 2, no lines cross the green line that would indicate good value with ETN as first therapy after MTX failure.

Sensitivity Analysis Showing No Cost-effectiveness With Etanercept
ETN, etanercept; HAQ, Health Assessment Questionnaire; ICER, incremental cost-effectiveness ratio; TT, triple therapy.
Reproduced with permission from N Bansback, PhD.
Interpreting the data, Dr Bansback noted that the use of biologics over the past 10 years has increased health care expenditures by tens of billions of dollars and that a considerable amount of money has been wasted by using biologics first instead of triple therapy. Biologics only appear to be cost-effective, he emphasized, after failure of triple therapy.
The consequence, concluded Dr Bansback, is that money from taxes, copays, deductibles, and premiums could have been saved or spent elsewhere to produce additional health on more interventions that are cost-effective.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.