

Summary
Recent publications were presented highlighting new molecular and genomic approaches for rapid diagnosis and susceptibility testing, and management of invasive fungal infections. Emphasis was on serum galactomannan assay and polymerase chain reaction–based detection of invasive Aspergillosis and other fungal infections in children and adults.
- fungal infections
- diagnostic strategies
- invasive Aspergillosis
- galactomannan assay
- voriconazole
- Candida glabrata
- caspofungin
- antifungal
- infectious diseases clinical trials
This session was devoted to a review of the most important recent papers in diagnostic and susceptibility testing, and management of fungal infections. Rosemary Barnes, MD, Cardiff University Institute of Infection and Immunity, Cardiff, United Kingdom, opened with her assessment of the top 10 recent studies describing diagnostic strategies and susceptibility testing.
The first study reviewed showed that a combined strategy of serum galactomannan (GM) assay and polymerase chain reaction (PCR)–based detection of serum Aspergillus DNA monitoring was associated with an earlier diagnosis and a lower incidence of invasive aspergillosis (IA) in high-risk hematologic malignancy and hematopoietic stem-cell transplant patients [Aguado JM et al. Clin Infect Dis. 2015].
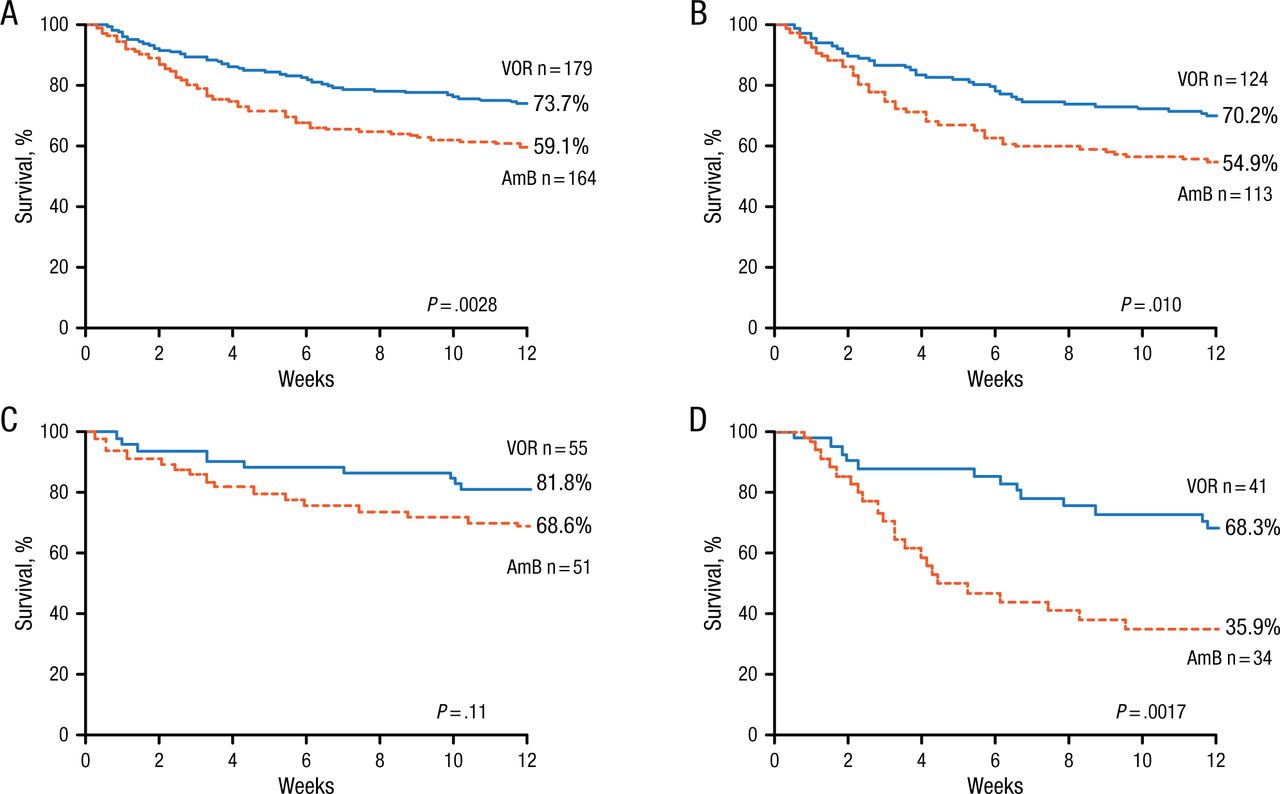
In the next study, which assessed definitions, the investigators found that using the European Organization for Research and Treatment of Cancer/Mycoses Study Group 2008 definitions of IA vs the earlier definitions from the Global Comparative Aspergillus Study resulted in a better classification of the episodes and confirmed the higher efficacy of voriconazole (VRC) over amphotericin B deoxycholate as initial therapy in mycologically documented IA (Figure 1) [Herbrecht R et al. Clin Infect Dis. 2015].

Voriconazole Improves 12-Week Survival Compared With AmB Deoxycholate
AmB, amphotericin B; IA, invasive aspergillosis; VOR, voriconazole.
A, possible, probable, and proven IA; B, probable and proven IA; C, possible IA; D, possible, probable, and proven IA in allogenic hematopoietic stem cell transplant recipients.
Reprinted from Herbrecht R et al, Application of the 2008 Definitions for Invasive Fungal Diseases to the Trial Comparing Voriconazole Versus Amphotericin B for Therapy of Invasive Aspergillosis: A Collaborative Study of the Mycoses Study Group (MSG 05) and the European Organization for Research and Treatment of Cancer Infectious Diseases Group. Clin Infect Dis, 2015; Vol 60; Issue 5: Pages 713-720, by permission of Oxford University Press on behalf of the Infectious Diseases Society of America.
The third study looked at patients with hematologic malignancies or hematopoietic cell transplantation having IA diagnosis established by radiographic findings and GM positivity and found these patients had better survival outcomes when treated with a combination of VRC and anidulafungin vs VRC monotherapy [Marr KA et al. Ann Intern Med. 2015].
The next group of studies focused on diagnostic approaches. In study 4, a rapid, noninvasive, pathogen-specific breath test for Aspergillus secondary metabolite signature successfully identified IA in patients with suspected fungal pneumonia [Koo S et al. Clin Infect Dis. 2014]. In study 5, PLEX-ID, a technique that uses PCR-electrospray ionization/mass spectrometry for rapid identification of infectious agents, was found to be not useful as a standalone tool for microbiological diagnosis in suspected respiratory infections and had limited impact on management of therapy [Huttner A et al. Clin Microbiol Infect. 2014]. Investigators in the next 2 studies determined that a microarray system using the internal transcribed spacer region of the rRNA gene amplified isothermally is an efficient and robust method for identifying a variety of fungal species [Sakai K et al. Mycopathologia. 2014] and that testing for urine GM as opposed to serum GM shows potential for IA screening [Duettmann W et al. Med Mycol. 2014].
Study 8 validated a new multiplex real-time PCR assay that allows for sensitive and fast detection of Aspergillus species directly from bronchoalveolar lavage (BAL) fluid samples [Chong GL et al. J Clin Microbiol. 2015]. This assay has the potential to detect and differentiate wild-type from azole resistant strains, even if BAL fluid cultures remain negative.
The last 2 studies focused on Candida. Study 9 reported the European Committee on Antimicrobial Susceptibility Testing method compared favorably with the Clinical and Laboratory Standards Institute method for generating minimum inhibitory concentration (MIC) values for most isolates of Candida [Pfaller MA et al. Diagn Microbiol Infect Dis. 2014]; meanwhile, in the final study to be reviewed, the investigators reported that of the current species-specific epidemiologic cutoff values (ECVs) for Candida glabrata, the current caspofungin ECV may not reproducibly differentiate resistant and susceptible C glabrata strains in hospitals with varying MIC distributions [Ben-Ami R et al. Diagn Microbiol Infect Dis. 2014].
Next, Souha S. Kanj, MD, American University of Beirut Medical Center, Beirut, Lebanon, discussed the top papers in the management of invasive fungal infections.
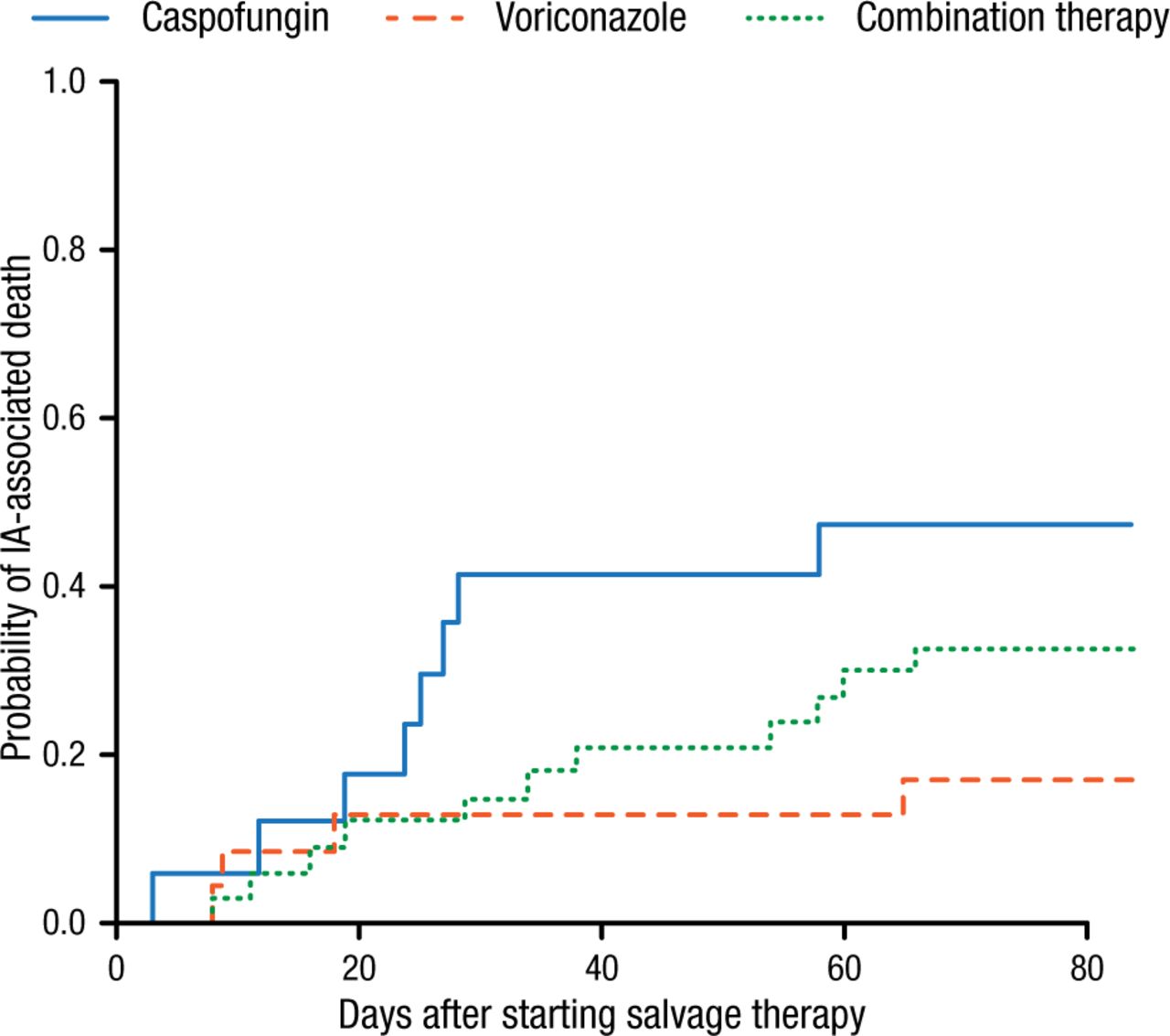
The first paper Prof Kanj reviewed was from a randomized controlled trial that included 454 patients with hematologic malignancies or hematopoietic stem cell transplantation and compared the safety and efficacy of VRC plus anidulafungin with VRC monotherapy [Marr KA et al. Ann Intern Med. 2015]. Mortality rates at 6 and 12 weeks were lower in the group that received combination therapy, but the results were not statistically significant. In a subgroup with positive GM, however, all-cause mortality was lower and statistically significant with combination therapy (P = .037). In contrast, the subsequent study in 181 patients with hematologic malignancies and IA who were treated with primary or salvage therapy with caspofungin, VRC, or the combination of both showed that for primary or salvage therapy, no difference in outcome was noted between combination treatment and VRC monotherapy [Raad II et al. Int J Antimicrob Agents. 2015]. However, in the salvage therapy group, VRC monotherapy led to lower Aspergillus-associated death compared with caspofungin monotherapy (Figure 2).

Probability of IA Deaths by Treatment in Salvage Therapy Group
P = .11; n = 75.
IA, invasive aspergillosis.
Reprinted from Int J Antimicrob Agents, Vol 45, Raad II et al, Clinical experience of the use of voriconazole, caspofungin or the combination in primary and salvage therapy of invasive aspergillosis in haematological malignancies, Pages 283-288, Copyright 2014, with permission from Elsevier.
The next study assessed the characteristics of IA caused by Aspergillus terreus in patients with hematologic malignancy [Hachem R et al. J Antimicrob Chemother. 2014]. The investigators noted that this form of A terreus has intrinsic or acquired resistance to amphotericin B, is associated with more breakthrough infections, and has a lower rate of final response to antifungal therapy and a higher rate of IA-associated mortality. It appears in younger patients more likely to have leukemia, but less likely to have lymphoma. Factors independently associated with IA death included treatment with azoles and having the A terreus vs non-terreus Aspergillus species.
The next 2 studies focused on candidiasis. In the first, investigators reported that preemptive (but not prophylactic) caspofungin treatment was safe and significantly reduced the incidence of proven or probable invasive candidiasis (P = .04; safety population only) when used in the intensive care unit [Ostrosky-Zeichner L et al. Clin Infect Dis. 2014]. The next study reported that 42 days of prophylactic fluconazole treatment compared with placebo did not reduce the incidence of composite death or invasive candidiasis in infants with a birth weight < 750 g [Benjamin DK Jr et al. JAMA. 2014].
In the last study Prof Kanj reviewed, the investigators reported that micafungin, prophylactically administered twice weekly at a dosage of 3 to 4 mg/kg of body weight in children at high risk for invasive fungal disease, may be a convenient, safe, and efficient alternative for antifungal prophylaxis [Bochennek K et al. J Antimicrob Chemother. 2015].
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.