

Summary
In selected symptomatic patients with suspected coronary artery disease, cardiac computed tomography coronary angiography combined with myocardial perfusion imaging provide complementary information about the structure and function of the heart. This improves the risk assessment and treatment decisions for these patients, compared with imaging alone.
- coronary artery disease
- positron emission tomography
- computed tomography
- myocardial perfusion imaging
- coronary artery calcium scoring
- cardiac computed tomography angiography
- cardiology & cardiovascular medicine screening & prevention
Many patients with normal myocardial perfusion assessed by positron emission tomography (PET)/computed tomography (CT) imaging have undetected coronary artery disease (CAD). Combining myocardial perfusion imaging (MPI) with coronary artery calcium scoring (CACS) improves the detection of CAD. Randall C. Thompson, MD, University of Missouri, Kansas City, Missouri, USA, discussed how the use of multimodality imaging often leads to the reclassification of a patient's risk for CAD and alters the course of treatment.
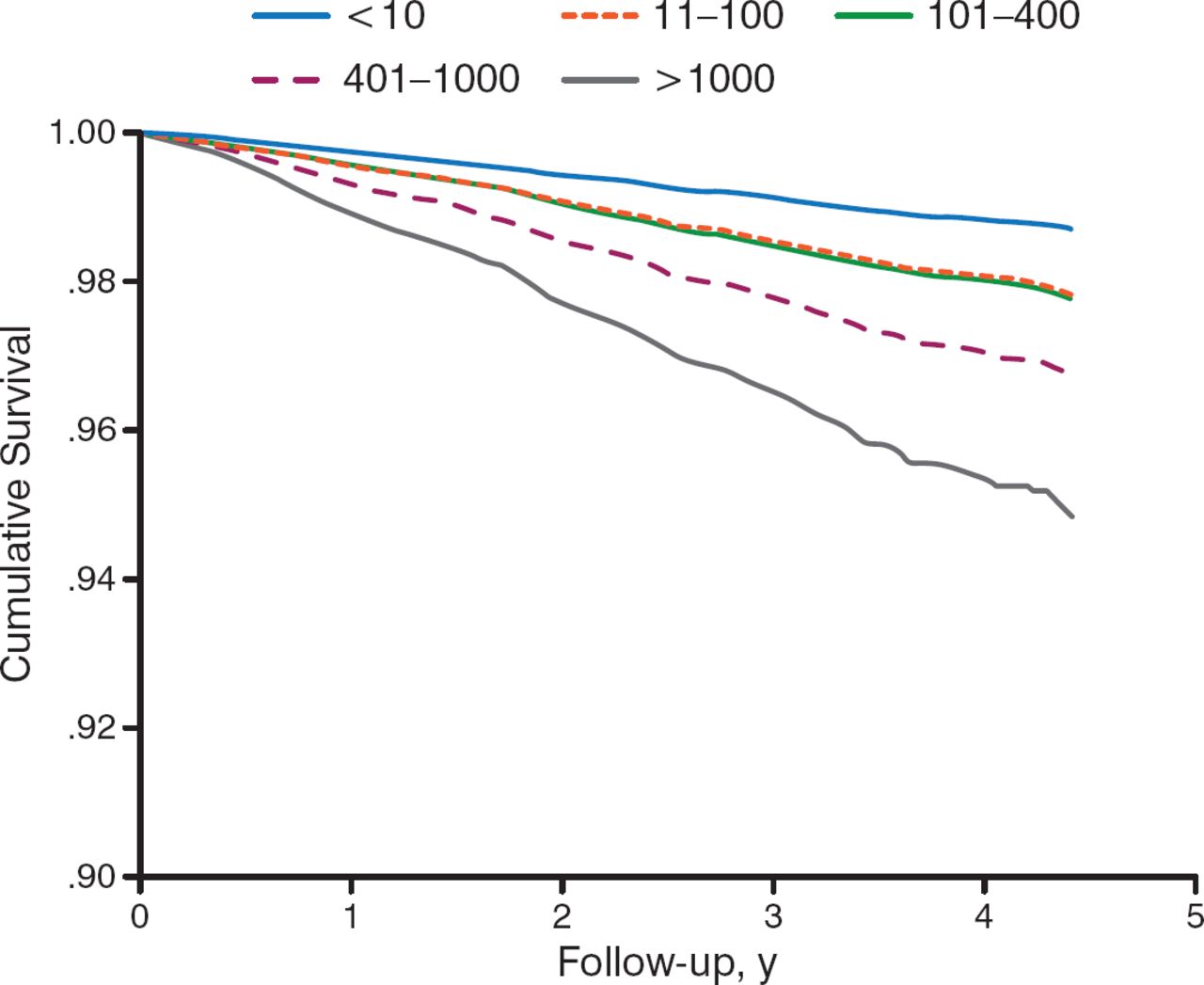
Patients with persistent symptoms and normal myocardial perfusion or mild ischemia on MPI are good candidates for CACS or cardiac computed tomography angiography (CCTA). CCTA can provide information about the amount of calcium in the walls of the coronary arteries and can help predict the risk of heart attack and cardiac death. The Agatston score, a measure of coronary calcification, is based on the area and density of calcified plaques and has been shown to be an independent predictor of mortality (P < .001; Figure 1) [Shaw LJ et al. Radiology. 2003].

Coronary Calcium Score Independent Predictor of All-Cause Mortality
Graph shows risk-adjusted all-cause survival estimates according to calcium score subsets. Even after adjustment, survival rate is proportionally worse as the baseline calcium score increases.
Adapted from Shaw LJ et al. Graph shows risk-adjusted all-cause sur vival estimates accord i ng to calcium score subsets. Even after adjustment, survival rate is proportionally worse as the baseline calcium score increases. Radiology, 2003;228:826–833. With permission from RSNA.
In one study, 200 patients without known CAD were referred for CACS after normal MPI. Based on a CAC score > 100, 17.5% were identified as having CAD. Patients who were reclassified by CACS were not easily identifiable by traditional risk factors, although the patient's age and Framingham risk score did predict the presence of CAC [Thompson RC et al. J Nucl Cardiol. 2005]. Another study of 760 patients with no CAD history, a normal PET/CT stress perfusion study, and a same-setting CAC scan found that 64.1% had subclinical CAD based on an abnormal CACS. Changes in medical therapy appeared to be related to whether the patient had received multimodal therapy (PET/CT) or dedicated PET [Bybee KA et al. J Nucl Cardiol. 2010].
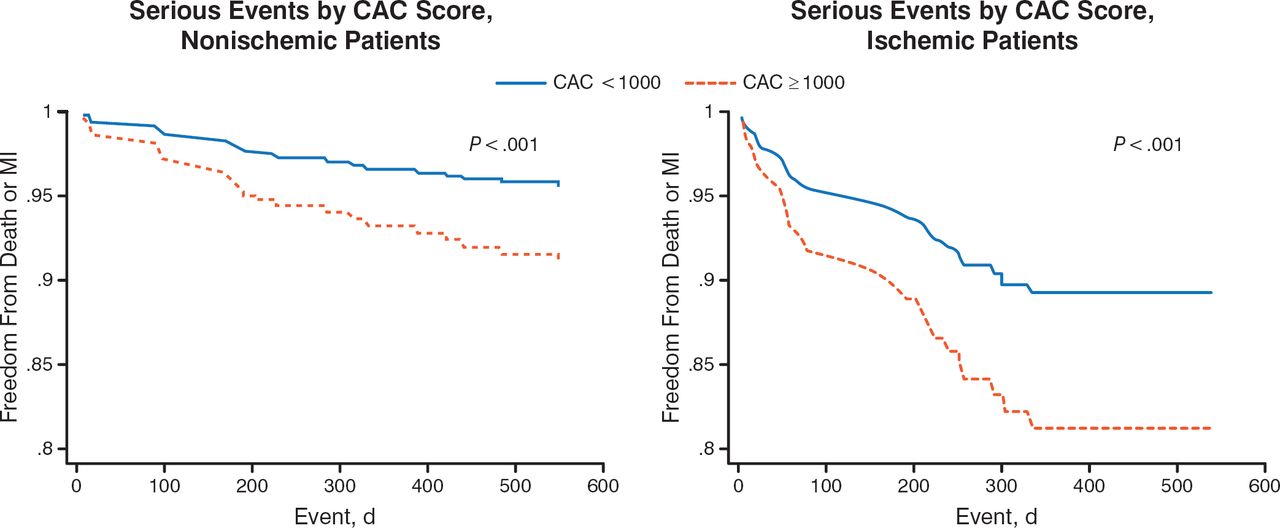
Although there was some residual risk of CAD in those with low CAC scores, higher CAC scores generally predicted a higher likelihood of ischemia. Annualized event rates in patients with normal PET MPI and no CAC were substantially lower than in patients with a CAC score ≥ 1000 (2.6% vs 12.3%). Rates were also lower among patients with ischemia on PET MPI and no CAC compared with those patients with a CAC score ≥ 1000 (8.2% vs 22.1%; Figure 2). These data suggest that incremental risk stratification can be achieved by incorporating information on the extent of CAD as measured by CACS, along with the physiological information gleaned from MPI [Schenker MP et al. Circulation. 2008].

High CAC Score Better Predictor of Poor Outcome Than Presence of Ischemia
CAC, coronary artery calcium; MI, myocardial ischemia.
Adapted from Schenker MP et al. Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: a combined positron emission tomography/computed tomography study. Circulation. 2008;117(13):1693–1700. With permission from American Heart Association.
MPI scans and computerized tomography coronary angiograms (CTCAs) have an internal link that provides good diagnostic performance for CAD [Li JM et al. Int J Mol Imaging. 2012]. They provide different and complementary information for detection of ischemia (MPI) versus detection of atherosclerosis (CTCA). There is concern, however, about the possibility of both false-positive and false-negative findings.
In patients with a negative MPI, 84.7% had a negative CTCA and 15.3% had a positive CTCA, whereas in patients with a positive MPI, 32.8% had a negative CTCA and 67.2% had a positive CTCA. In contrast, in patients with a negative CTCA, the proportion with a negative and positive MPI were 94.4% and 5.6%, respectively, whereas in patients with a positive CTCA, these proportions were 59.8% and 40.2%, respectively.
Multiple studies have noted that the frequency of ischemia in vessels with ≥ 50% stenosis (detected by CTA) had a negative predictive value of 91% to 100% and positive predictive value of 29% to 44%. Dr Thompson advises using MPI to confirm ischemia when stenosis is identified on a coronary CTA. MPI improves the detection of CAD in vessels < 2 mm, whereas CTA contributes to the assessment of multivessel CAD. One advantage of MPI with a hybrid CT device is the ability to obtain same-setting measurement of the CACS, which makes it possible to detect obstructive atherosclerosis causing myocardial ischemia. Both techniques contribute to the management of coronary stenosis.
In best practice, the routine addition of CACS to MPI improves the detection of disease in patients who merit medical CAD management and prevention strategies. Patients who have normal or mildly ischemic MPI and persistent symptoms are good candidates for CACS or CCTA. Patients with indeterminate, or even severe, lesions on CCTA frequently merit additional testing with MPI, CT angiography with fractional flow reserve for detecting ischemia, and CT MPI.
An anatomy-based testing strategy with CT coronary angiography and a physiology-based testing strategy with MPI may be clinically useful for the evaluation of known or suspected CAD in symptomatic patients. In selected patient cohorts, imaging approaches integrating structure and function may provide improved assessments of risk, thereby allowing a more personalized approach to management.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.