

Summary
This article gives an overview of obstructive sleep apnea (OSA) as a risk factor for cerebrovascular disease and stroke [Culebras A, editor. Sleep, Stroke and Cardiovascular Disease. Cambridge University Press, 2013].
- Episodic & Paroxysmal Disorders
- Sleep Disorders
- Episodic & Paroxysmal Disorders
- Sleep Disorders
- Neurology
Antonio Culebras, MD, SUNY Upstate Medical University, Syracuse, New York, USA, provided on overview of obstructive sleep apnea (OSA) as a risk factor for cerebrovascular disease and stroke [Culebras A, editor. Sleep, Stroke and Cardiovascular Disease. Cambridge University Press, 2013].
Sleep apnea may contribute to cerebrovascular disease in a variety of ways (Table 1).
Sleep Apnea-Related Contributors to Cerebrovascular Disease
SLEEP APNEA-RELATED HYPERTENSION
The regularity of arousals from apnea influences hypertension [Jamasebi R et al. Sleep 2008]. The Sleep Heart Health Study reported a progressive increase in adjusted odds of hypertension with ≥15 episodes of apnea per hour [Nieto FJ et al. JAMA 2000].
CARDIAC ARRHYTHMIA
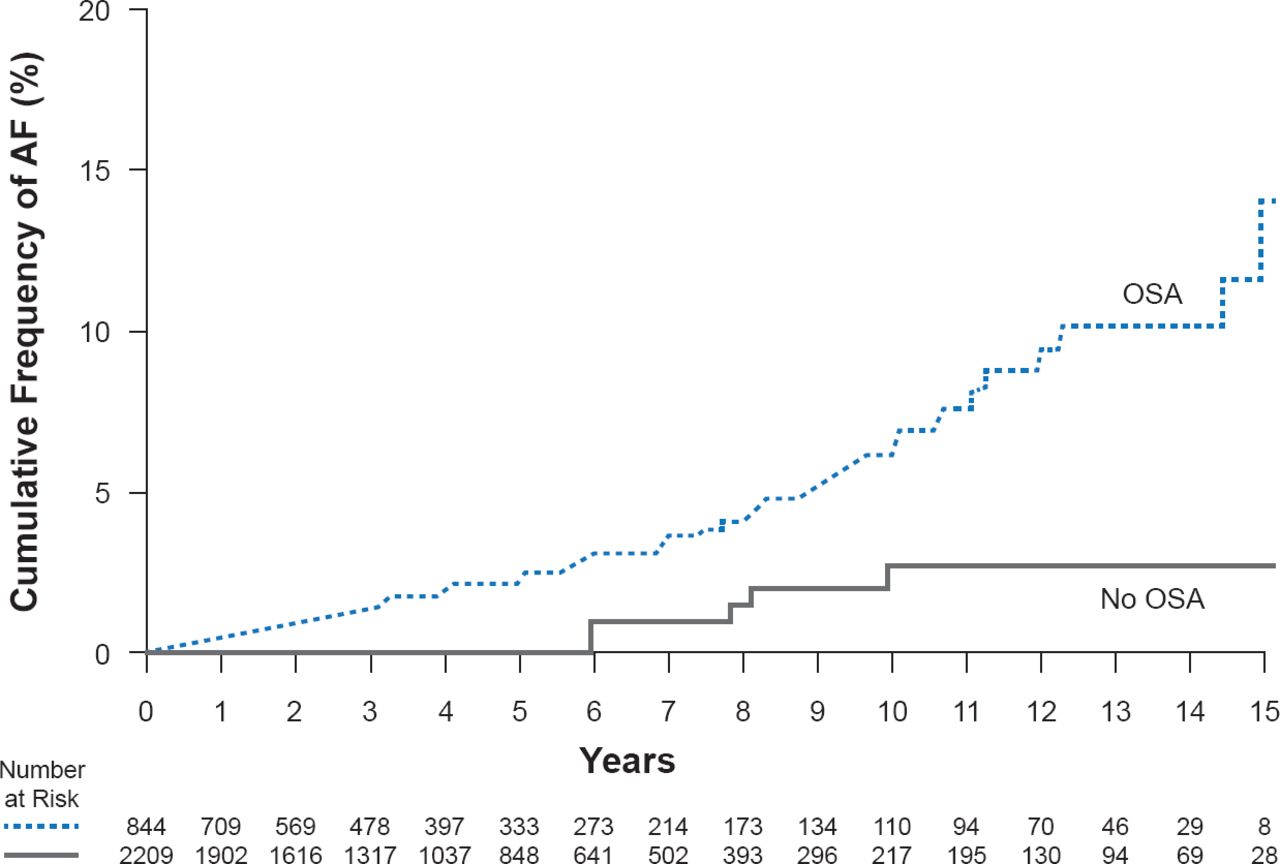
Many atrial fibrillation (AF) episodes (40%) occur during the typical sleep period (midnight to 8:00 AM) and AF risk increases nearly 3-fold with sleep apnea-mediated decreases in blood oxygen. Sleep apnea is significantly more prevalent (p=0.0004) in patients with AF (49%) than in patients with other cardiovascular diseases who are at high-risk for AF (32%) [Gami AS et al. Circulation 2004], and significantly more frequent in those with AF compared with age-matched healthy individuals (81.6% vs 60%; p=0.03) [Braga B et al. Sleep Med 2009]. OSA is a univariate predictor of AF (Figure 1) [Gami AS et al. J Am Coll Cardiol 2007].

Cumulative Frequency of AF for Subjects With and Without Obstructive Sleep Apnea
OSA=obstructive sleep apnea.
Reproduced from Gami AS et al. Obstructive Sleep Apnea, Obesity, and the Risk of Incident Atrial Fibrillation. J Am Coll Cardiol 2007;5(6):565–571. With permission from Elsevier.
PATENT FORAMEN OVALE
Patent foramen ovale has been significantly associated (p<0.05) with sleep apnea in 27% of subjects compared with 15% of subjects with a normal heart [Beelke M et al. Sleep Med 2003]. The presence of right-to-left shunt in 72% of 100 consecutive patients with OSA [Guchlerner M et al. J Clin Sleep Med 2012] is evidence of an association of patent foramen ovale with sleep apnea. In a study of 335 patients, OSA lasting ≥20 seconds was associated with wake-up strokes and transient ischemic attack in patients with right-to-left shunt (27/69) compared with patients with apnea alone (70/266; OR, 1.91; 95% CI, 1.08 to 3.38; p=0.03) [Ciccone A et al. Thorax 2013].
The data to date supports the suggestion that OSA significantly increases the risk of stroke or death from any cause, independent of other risk factors including hypertension [Yaggi HK et al. N Engl J Med 2005]. Additionally, apnea has been linked to cognitive impairment [Yaffe K et al. JAMA 2011; Román GC et al. Lancet Neurol 2002].
Therapeutic use of continuous positive airway pressure has been explored in OSA. Encouraging findings include lowered cardiovascular risk [Kohler M et al. Eur Respir J 2008], decreased blood pressure [Jaimchariyatam N et al. Sleep Med 2010; Martínez-García MA et al. Eur Respir J 2007], and potential value in reducing mortality [Martínez-García MA et al. Am J Respir Crit Care Med 2009].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.