

Summary
Multiple vasculopathies other than atherosclerosis can cause the narrowing or occlusion of arteries, and while they have some overlapping symptoms, they also have distinct characteristics that providers should use to reach a differential diagnosis. This article discusses Moyamoya disease, reversible cerebral vasoconstriction syndromes, and central nervous system vasculitis.
- Vasculitis
- Episodic & Paroxysmal Disorders
- Ischemia
- Vasculitis
- Episodic & Paroxysmal Disorders
- Ischemia
- Neurology
Multiple vasculopathies other than atherosclerosis can cause the narrowing or occlusion of arteries, and while they have some overlapping symptoms, they also have distinct characteristics that providers should use to reach a differential diagnosis. Gary K. Steinberg, MD, PhD, Stanford University School of Medicine, Stanford, California, USA, discussed Moyamoya disease, a progressive disease of the internal carotid artery that results in occlusion, causing in decreased blood flow to the brain. As a result, the small vessels in the brain become enlarged and may hemorrhage.
Prior treatments for Moyamoya disease included medical management with antiplatelet and anticoagulant agents, steroids, vasodilators, mannitol, and calcium channel antagonists. None of these therapies have been shown to be effective. However, surgical revascularization using extracranial to intracranial bypass grafts is effective as it improves cerebral perfusion and reduces stress on collateral vessels. The rate of symptomatic progression with surgical therapy is 2.7% [Fung LW et al. Childs Nerv Syst 2005] compared with 20% to 65% with medical therapy [Hallemeier CL et al. Stroke 2006; Chiu DS et al. Stroke 1998].
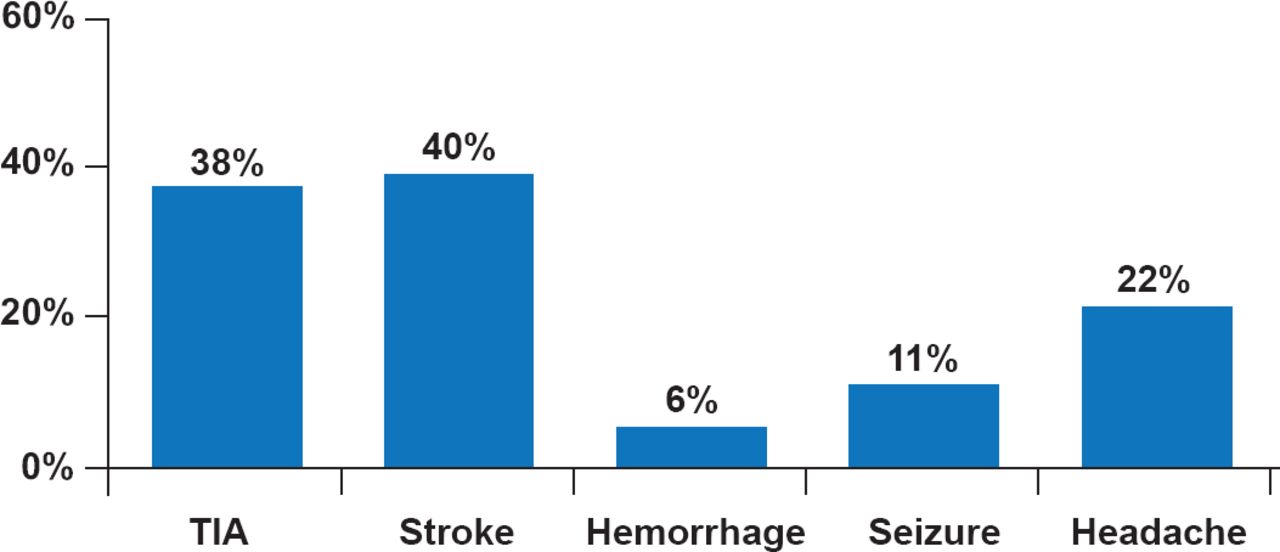
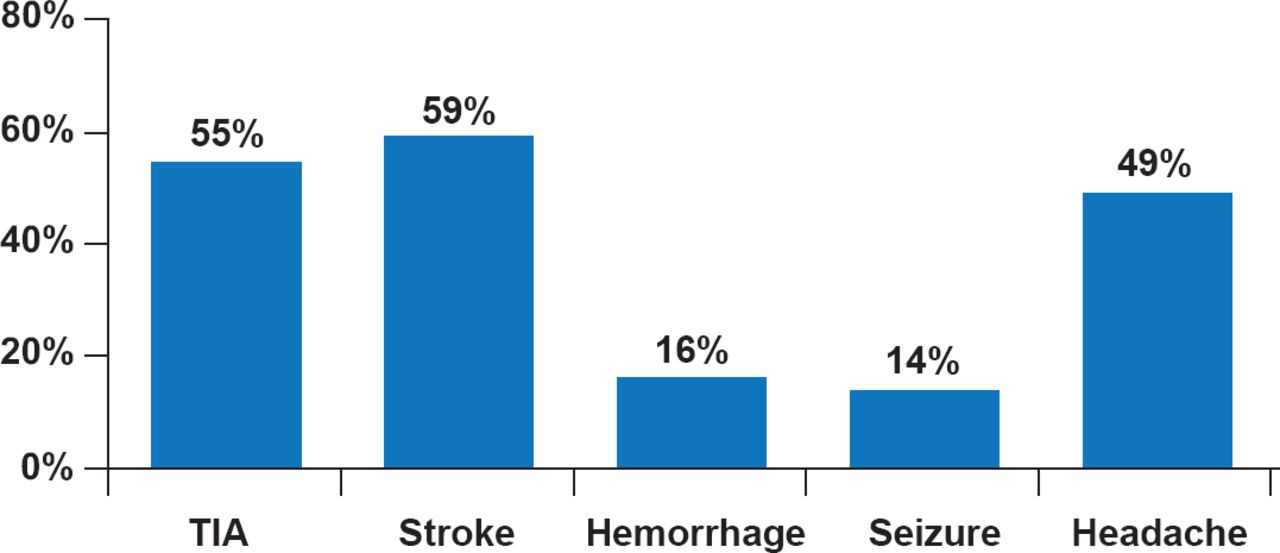
The Stanford Moyamoya Series includes 716 adult and pediatric patients who were recruited across the United States and internationally between 1991 and 2014. In pediatric and adult patients, the most common presenting symptoms are stroke, transient ischemic attack (TIA), and headache (Figures 1 and 2). Moyamoya disease is underdiagnosed and can be misdiagnosed as multiple sclerosis [Dorfman LI et al. Neurologist 2012].

Common Symptoms of Moyamoya Disease in Children
TIA=transient ischemic attack.
Reproduced from Dorfman LJ et al. Moyamoya disease can masquerade as multiple sclerosis. Neurologist 2012; 18(6):398–403. With permission from Lippincott Williams and Wilkins.

Common Symptoms of Moyamoya Disease in Adults
TIA=transient ischemic attack.
Reproduced from Dorfman LJ et al. Moyamoya disease can masquerade as multiple sclerosis. Neurologist 2012;18(6):398–403. With permission from Lippincott Williams and Wilkins
One method of direct revascularization is the anastomosis of the superficial temporal artery in the scalp to the M4 branch of the middle cerebral artery within the brain. Another method that is particularly effective in children is indirect revascularization. The blood vessel is isolated within the scalp, the underlying bone is removed, and the intact artery is then placed on the surface of the brain. Over the course of about 3 to 6 months, new vasculature will connect to the artery to the brain. Omental-cerebral transposition is another indirect revascularization method in patients for whom other methods fail, where the omentum is lengthened by dissecting it from the greater curvature of the stomach, yet is still attached to the gastroepiploic artery, and is stretched to the brain, where it revascularizes the brain. To reduce morbidity, isolation of the omentum is now performed laparoscopically. However, Dr. Steinberg stated that, in his opinion, indirect revascularization is not always as effective as direct revascularization.
Long-term results of 450 revascularization procedures in 264 patients from the Stanford Moyamoya Series over a mean follow-up period of 4.9 years demonstrated that the 5-year risk of experiencing stroke was 5.5% after revascularization surgery [Guzman R et al. J Neurosurg 2009]. Of the 171 patients initially presenting with TIAs, 82.5% were TIA free at 1 month and 91.8% at 1 year following revascularization.
Aneesh B. Singhal, MD, Harvard Medical School, Boston, Massachusetts, USA, discussed reversible cerebral vasoconstriction syndromes (RCVS). Elements for diagnosis include multifocal cerebral vasoconstriction, “thunderclap” headache, normal or near-normal cerebrospinal fluid (CSF) results, and the absence of aneurysmal subarachnoid hemorrhage (SAH) [Calabrese LH et al. Ann Intern Med 2007]. In addition, reversibility must be documented and diseases with similar symptoms should be ruled out. The clinical course of RCVS is typically self-limiting and benign.
The process of diagnosing RCVS includes clinical recognition based on recurrent thunderclap headaches, characteristic brain imaging findings, and the typical ‘sausage-on-a-string’ appearance of cerebral arteries on angiography. Although there may be some overlap, RCVS and migraine headache are distinct conditions. Migraine frequently recurs over decades, whereas an episode of RCVS typically does not recur.
RCVS and aneurysmal SAH have overlapping features as well, including thunderclap headache, SAH, seizures, delayed infarcts, and cerebral artery narrowing. In a recent study, patients with RCVS were more likely to have a prior headache disorder, history of depression, or chronic obstructive pulmonary disease compared with patients that suffered from aneurysmal SAH (Table 1) [Muehlschlegel S et al. JAMA Neurol 2013]. In addition, patients with RCVS were more likely to be of younger age, female, have a history of hypertension, and have had a prior headache disorder, compared with patients that suffered from cryptogenic SAH.
Features Associated With RCVS Compared With Aneurysmal or Cryptogenic SAH
Primary angiitis of the central nervious system (PACNS) is an important differential diagnosis. However, there are features that are very distinct between RCVS and PACNS such as type of headache, infarct pattern, and presence of convexal SAH or brain edema (Table 2).
Distinguishing Features of RCVS and PACNS
Dr. Singhal stated that simple observation should be the primary management strategy. When treating RCVS, providers should avoid further exposure to vasoconstrictive agents and avoid blood pressure modulating agents, as these drugs can precipitate stroke or theoretically worsen the vasoconstriction. Intravenous fluids, pain management, and measures to avoid the Valsalva maneuver (eg, laxatives) are important. In one large retrospective study, steroid use was significantly associated with poor outcome, defined as a discharge mRS score >3. Nearly half the patients who received steroids developed new symptoms or infarcts within 2 to 6 days of treatment [Singhal AB et al. Arch Neurol 2011]. Dr. Singhal pointed out that steroids may have been initiated in these patients since they were already showing clinical progression (although chart review did not indicate this was the case). Yet, this study highlights that while steroids may not do harm, they likely do not provide a true benefit. Intra-arterial vasodilators can result in immediate reversal of arterial narrowing in RCVS but not in mimics such as PACNS and intracranial atherosclerosis. Hence, intra-arterial infusion of vasodilators is being proposed by some authors as a diagnostic test to rule out vasculitis. However, Dr. Singhal warns against the routine use of nicardipine because most cases of RCVS can easily be easily diagnosed at the bedside based on clinical and imaging features alone, and RCVS can be easily differentiated from mimics such as PACNS. Moreover, most RCVS cases are benign, whereas intra-arterial vasodilation incurs the risk of adverse events, such as reperfusion injury and rebound vasoconstriction
Rula Hajj-Ali, MD, Cleveland Clinic, Cleveland, Ohio, USA, discussed CNS vasculitis, a rare heterogeneous disease with many subsets which, if detected early, is treatable. When CNS vasculitis is confined to the brain, it is referred to as PACNS. If there is systemic involvement, then the vasculitis is secondary. Symptoms include chronic, insidious headache with multiple focal deficits. Angiograms are frequently negative because the resolution of the angiogram is not sufficient for detection. In one subset, 5% present with mass-like lesions, and the pathology of the tumors is lymphocytic inflammation [Molloy ES et al. Ann Rheum Dis 2008]. In these cases, it is important to rule out CNS lymphoma. About 7% to 8% of patients [Salvarani C et al. Ann Neurol 2007] with PACNS have associated amyloid β peptide (Aβ)-related angiitis which may present with multiple hemorrhages [Scolding NJ et al. Brain 2005].
Although a positive biopsy or angiogram suggestive of vasculitis can indicate a diagnosis of CNS vasculitis, Dr. Hajj-Ali stated that the most important element of diagnosis is to rule out other conditions that can cause a positive biopsy or angiogram. In addition, it is important to evaluate the CSF in patients suspected of having CNS vasculitis because it can rule out infection or malignancy. The preferred tool for nonvascular imaging is magnetic resonance imaging (MRI). Although the changes seen by MRI are generally nonspecific, a normal MRI is rarely seen in patients with CNS vasculitis. Dr. Hajj-Ali pointed out that if a patient's MRI and CSF sample are normal but the angiogram is abnormal, the patient likely has RCVS instead of CNS vasculitis.
Ranging from benign to a fatal natural course, nonatherosclerotic vasculopathies may have similar symptoms; however, they also have distinct features that can be used to reach a differential diagnosis. In any case, it is important to order a sufficient work-up so that an accurate diagnosis can be achieved.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.