

Summary
Carotid endarterectomy has been utilized to treat atherosclerosis of the carotid arteries for over 50 years. The advent of carotid artery stenting provided another option for treating these blockages. The number of imaging modalities that is available to physicians in the management of this condition continues to expand. This article reviews current medical evidence surrounding the management of carotid artery sclerosis using these two methods.
- neuroimaging
- dementias
- thrombotic disorders
- ischemia
- interventional radiology
- interventional techniques & devices
Carotid endarterectomy (CEA) has been utilized to treat atherosclerosis of the carotid arteries for over 50 years. The advent of carotid artery stenting (CAS) provided another option for treating these blockages. This symposium reviewed current medical evidence surrounding the management of carotid artery sclerosis using these two methods.
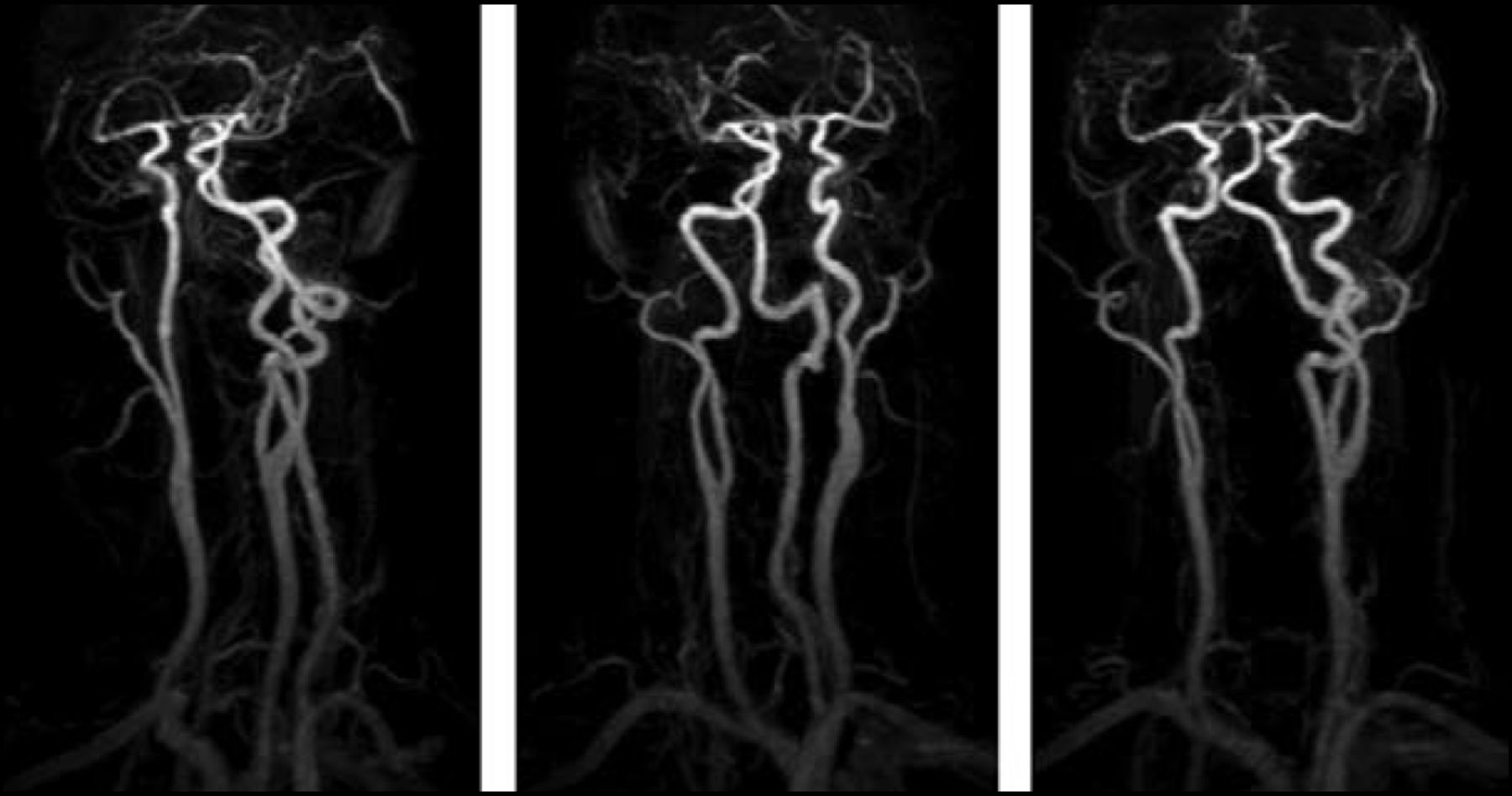
The number of imaging modalities that is available to physicians in the management of this condition continues to expand. Jeffrey Sunshine, MD, PhD, Case Western Reserve University, Cleveland, OH, briefly reviewed the characteristics of these technologies. Time-of-flight magnetic resonance angiography (MRA) takes 3–7 minutes and delivers a clear picture of carotid stenosis. MRA that is enhanced with a gadolinium bolus has an excellent contrast-to-noise ratio and a wide field of view. “You can see from the arch through the skull base, the entire carotid system…it's a tremendous dataset,” said Dr. Sunshine (Figure 1). The downside is that noninvasive technologies can overestimate stenoses. For this reason, “it is recommended that you get concordance with at least 2 studies to demonstrate high-grade stenoses,” said Dr. Sunshine.

CE MRA- Large View of MIPs.
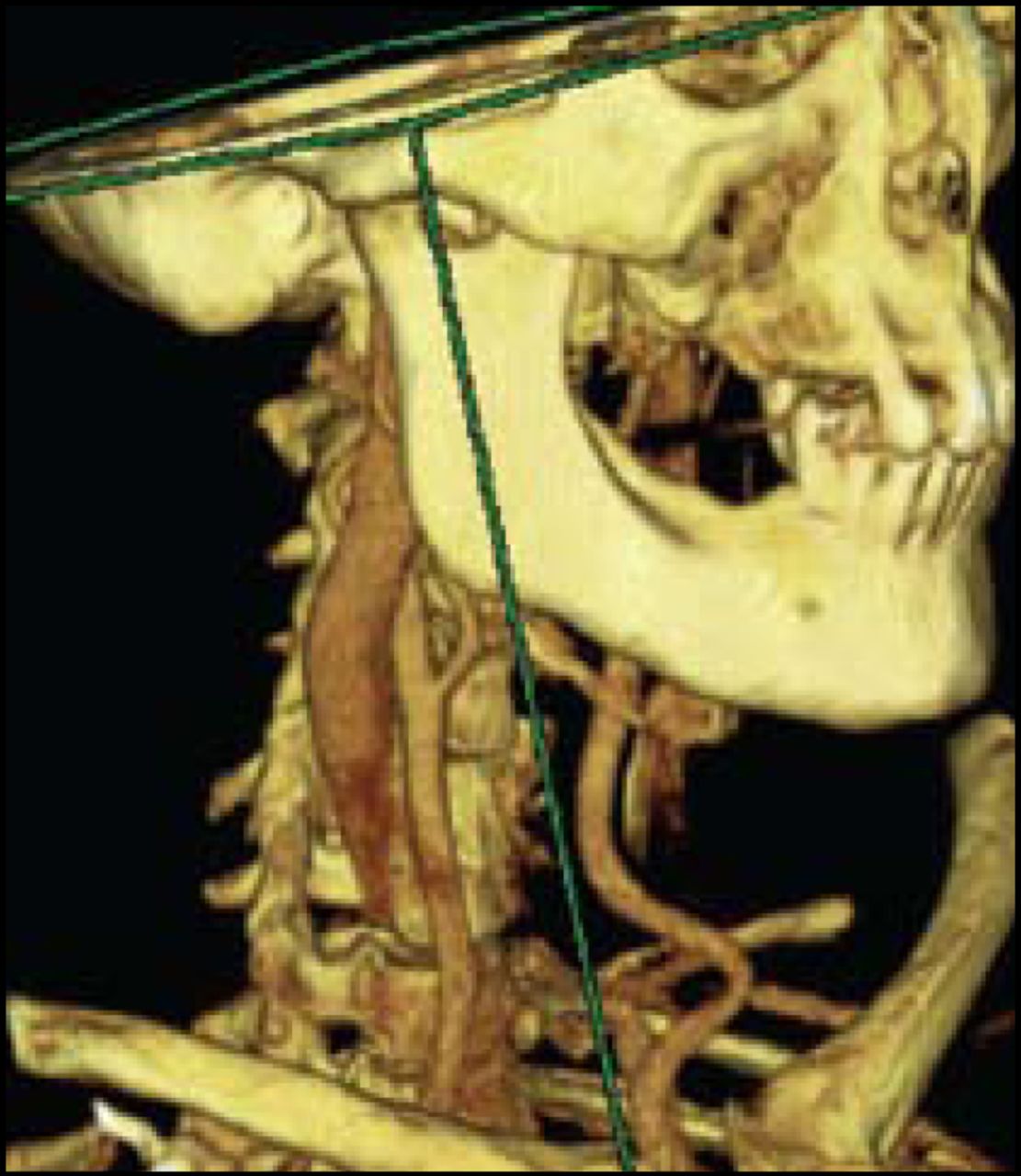
Ultrasound is operator-dependent and cost-effective, and remains “a mainstay of carotid imaging.” When combined with MRA, ultrasound results in 100% sensitivity and 80% specificity; concordance was found in 80% of patients. “There still remain false positives, and therein lies the problem with all noninvasive imaging,” commented Dr. Sunshine. Computed tomography angiography has the highest spatial resolution a large field of view, provides the best visualization of calcifications, and may allow visualization of the distal arteries (Figure 2). Catheter angiography remains a standard technology, allowing diagnosis and CAS to be performed in the same procedure in appropriate patients. Future directions of imaging research include 3-dimensional ultrasound, Doppler ultrasound for possible emboli, MRI detection of shear stress, and external phased-array MR imaging of plaque.

CTA.
L. Nelson Hopkins, MD, University of Buffalo, Buffalo, NY, believes that clinicians should use a comprehensive decision-making process when determining whether a patient should undergo CEA or CAS for carotid atherosclerosis. In his opinion, elderly patients should be offered treatment for this condition based on risk factor assessment. For example, if a patient is asymptomatic, is elderly, has a life expectancy >5 years, and is at low risk for either CEA or CAS, then treatment should be given. Dr. Hopkins' team reviews each patient and their risk factors in order to determine the best course of action. Approximately 20% of patients are at high risk for CEA. CAS may be a better option in those patients who are known to be at increased risk for CEA, assuming they do not have significant risk factors for CAS, it is best to “consider all the issues. If one [procedure] is high-risk, the other is probably not.” Dr. Hopkins provided the following factors that should be considered in the decision-making process:
The stent technology continues to evolve, and tools that provide distal and proximal embolic protection have been an important addition to CAS procedures. “We're getting smarter, we're getting better, and we're getting better technology…let's stop all the arguing and focus on what procedure is best for a given patient,” concluded Dr. Hopkins.
E. Sander Connolly, MD, Columbia University, New York, NY, gave an overview of neurocognitive dysfunction that is observed in patients after they have undergone CEA or CAS. Dr. Connolly and colleagues use a neurocognitive battery that consists of the Boston Naming test, the Controlled Oral Word Association test, the Halstead-Reitan Trails test (Parts A and B), and the Rey Complex Figure test. Measuring cognitive performance is complicated by the dynamic nature of the disease: some will improve after CEA and some will worsen. For this reason, researchers have chosen 24 hours post-procedure as the best time to collect measurements. The data that have been generated to date indicate that cognitive dysfunction occurs in approximately 25% of patients undergoing CEA. This effect is not related to general anesthesia, because this type of decline was not evident in control groups of awake CEA patients and patients undergoing coronary artery stenting. This type of injury is also observed in patients undergoing CAS. The injury that causes this decline in cognitive performance may be due to regional hypoperfusion in CEA (Heyer et al. Neurology 2006) and microembolism in CAS (Poppert et al. J of Neurol 2004). Certain patients appear to be at higher risk for this cognitive decline. Age (odds ratio 2.57; p=0.05) and diabetes mellitus (OR 4.26; p=0.03) were positive predictors for cognitive decline after CEA (Mocco et al. Neurology 2006), as well as a high monocyte count prior to surgery (OR 2.37; p<0.01; Mocco et al. Stroke 2006) and apolipoprotein E epsilon4 allele positivity (OR 62.28; p=0.007;Heyer et al. Neurology 2005).
A dose-ranging pilot study with magnesium sulfate was conducted to determine if patients could be protected from this cognitive injury. Results indicated that the low dose (2 mg loading dose followed by 8- or 16 mg infusion) appeared to protect patients (OR 0.27; p<0.01) when compared with the higher dose (4 mg loading dose + 16 mg infusion) or saline placebo. “If you look at patients who had magnesium infusions in an obstetrical situation, they have decreased attention and working memory levels achieved in this trial (Ghia et al. Am J Obstet Gyn 2000). Even though high-dose magnesium may be more protective, it clouds the measurement tool we are using in these trials,” commented Dr. Connolly. These findings have led to plans for a larger study that will hopefully result in better management of patients undergoing CEA or CAS.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.