

Summary
Patients who suffer strokes experience residual symptoms in many areas. Reports in the literature indicate that 38% of patients reported major difficulty in hand function 1–3 months post-stroke
- extrapyramidal & movement disorders
- cerebrovascular disease
Patients who suffer strokes experience residual symptoms in many areas. Reports in the literature indicate that 38% of patients reported major difficulty in hand function 1–3 months post-stroke (Duncan et al. Stroke 2003), and up to 65% of patients could not use their paretic hand in daily activities 6 months post-stroke (Mayo et al. 2002). “The impact of manual function on independent living is significant…this is one of the precursors of losing independent capability,” said Carolee Winstein, PhD, PT, University of California, Los Angeles, CA. Different approaches are being explored to help alleviate post-stroke disability, and studies suggest that intensive, task-oriented upper limb training (TOULT) may be effective. The Stroke Arm Recovery (STAR) trial was a phase 2, unblinded, single-center study that compared TOULT, strength training (ST), and standard care (SC) on upper limb recovery. The TOULT group was significantly better than the SC group in measures of impairment (p=0.04) and strength (p=0.02). Nine months later, the less severe stroke patients outperformed the ST group in strength (p<0.05; Winstein et al. Arch Phys Med Rehabil 2004). In the phase 3 Extremity Constraint-Induced Therapy Evaluation (EXCITE) trial, 222 stroke patients were randomized to receive either constraint-induced movement therapy (CIMT) or SC 3–9 months post-stroke. Patients who received CIMT had statistically significant, clinically relevant improvements that lasted for at least one year (Wolf et al. JAMA 2006). “The critical elements of constraint therapy remain unresolved. Is it the task-oriented training, is it the shaping repetition, is it the forced use?” commented Dr. Winstein. These questions are in need of additional research.
Electromagnetic brain stimulation methodology and its potential effect on motor stimulation training were reviewed by Leonardo Cohen, MD, National Institutes of Health, Bethesda, MD. “One line of evidence that has been demonstrated so far…is that when different forms of brain stimulation are applied over the primary motor cortex (M1), there is a resultant increase in motor cortical excitability,” said Dr. Cohen. This led to the idea that stimulation may provide a synergistic effect on motor training in humans, and emerging technologies are in the proof-of-concept stage (Hummel FC, Cohen LG. Lancet Neurology 2006). The types of issues that need resolution include optimization of the stimulation site, technique optimization, characterization of the patients/injuries/tasks that may be helped, and the safety of the procedures (Tallelli P, Rothwell J. Curr Opin Neurol 2006; Fregni F, Pascual-Leone A. Cogn Behav Neurol 2006).
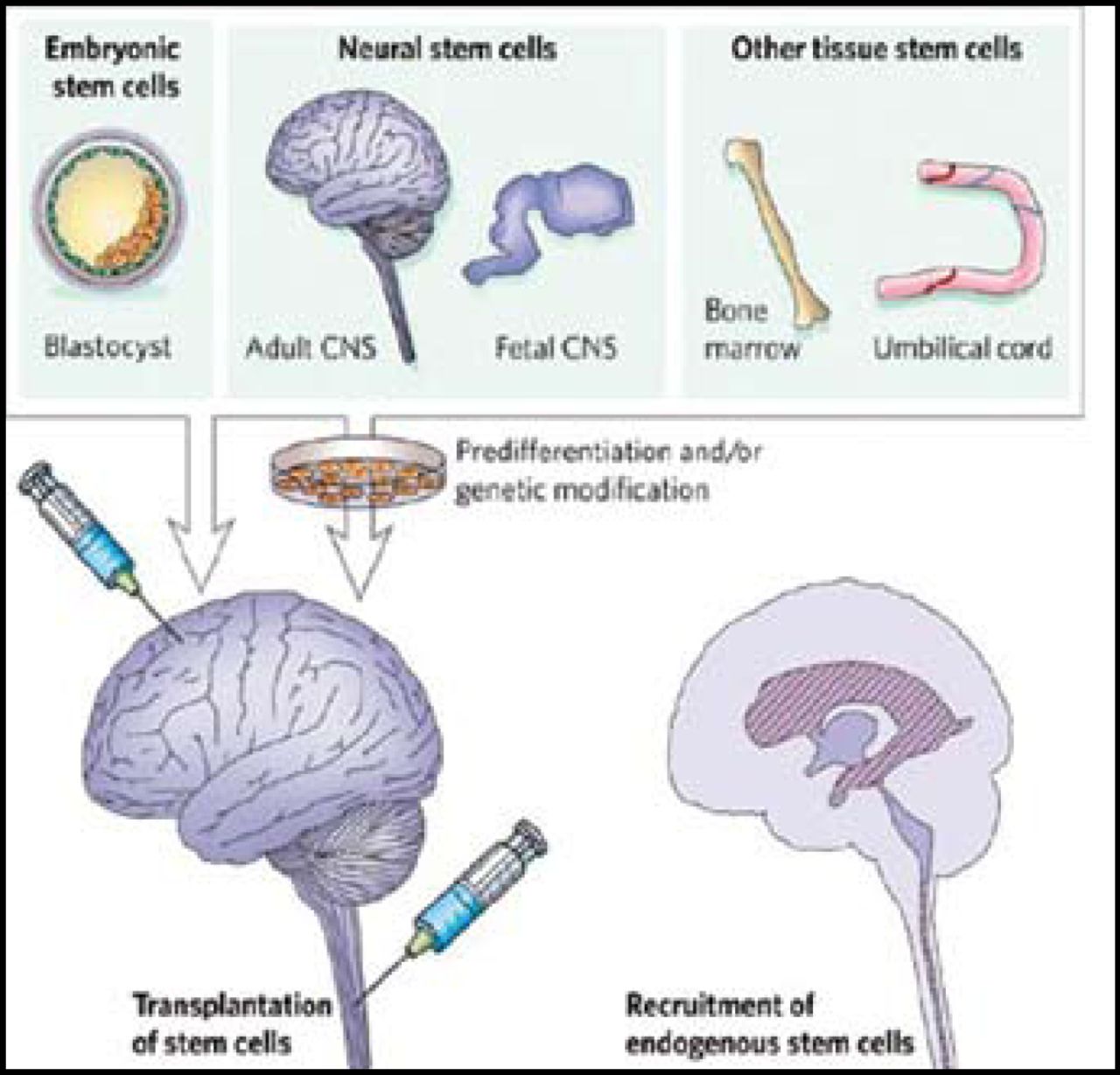
Cellular therapies are also being explored as a mechanism for brain repair after stroke, as discussed in an overview given by Sean Savitz, MD, University of Texas, Houston, TX. The concept arose from stem cell transplantation in cancer patients as well as transplantation in those with Parkinson disease. Promotion of lost neuronal connections and conductivity, enhancement of trophic support for neurogenesis, angiogenesis, synaptogenesis, prevention of cell death, and reduction of inflammatory responses and scar formation are some of the possible mechanisms whereby cell therapy could enhance brain recovery. Although it is an exciting idea, it is an area that is full of challenges. “Is it really possible to consider that cellular therapy or cellular transplantation is going to reconstruct the complex tapestry of the infarcted brain?” asked Dr. Savitz. Some of the parameters that researchers must determine are the infarct size and location, the timing of therapy, injection sites, routes of delivery, which cell types (Figure 1), and patient safety monitoring. The search for an effective therapy to promote brain repair after stroke continues to evolve across the domains of physical therapy, brain stimulation, and cell therapy.

Complexity of Cell Types.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.