

Summary
Blood pressure (BP) is a surrogate that is treated to prevent cardiovascular disease (CVD) and its consequences. However, outside of clinical trials, it is difficult to know how these outcomes are affected by antihypertensive therapy. Although clinical trials provide useful information, they do not give the full picture. Real-life practice is more complicated than clinical trials, but both need to be considered in managing hypertension (HTN). This article discusses the new international guidelines for the management of HTN were issued in Europe and the United States in 2013.
- Hypertensive Disease
- Cardiology Guidelines
- Hypertensive Disease
- Cardiology Guidelines
- Cardiology
Alistair Hall, MD, Leeds Institute of Cardiovascular and Metabolic Medicine, Leeds, United Kingdom, reminded the audience that blood pressure (BP) is a surrogate that is treated to prevent cardiovascular disease (CVD) and its consequences. However, outside of clinical trials, it is difficult to know how these outcomes are affected by antihypertensive therapy. Although clinical trials provide useful information, they do not give the full picture. Real-life practice is more complicated than clinical trials, but both need to be considered in managing hypertension (HTN).
New international guidelines for the management of HTN were issued in Europe and the United States in 2013. Both the American Society of Hypertension and the International Society of Hypertension guidelines attempted to be practical but were criticized as opinion pieces that were not developed using a formal guideline process [Weber MA et al. J Clin Hypertens 2013].
The Eighth Joint National Committee (JNC 8) guidelines claimed to be a scientific advisory document but were criticized for being excessively stringent [James PA et al. JAMA 2013]. According to Prof. Hall, the European Society of Hypertension (ESH) and European Society of Cardiology (ESC) guidelines allow for clinical opinion [Mancia G et al. Eur Heart J 2013]. All 3 sets of guidelines agree that the recommendations are not a substitute for clinical judgment.
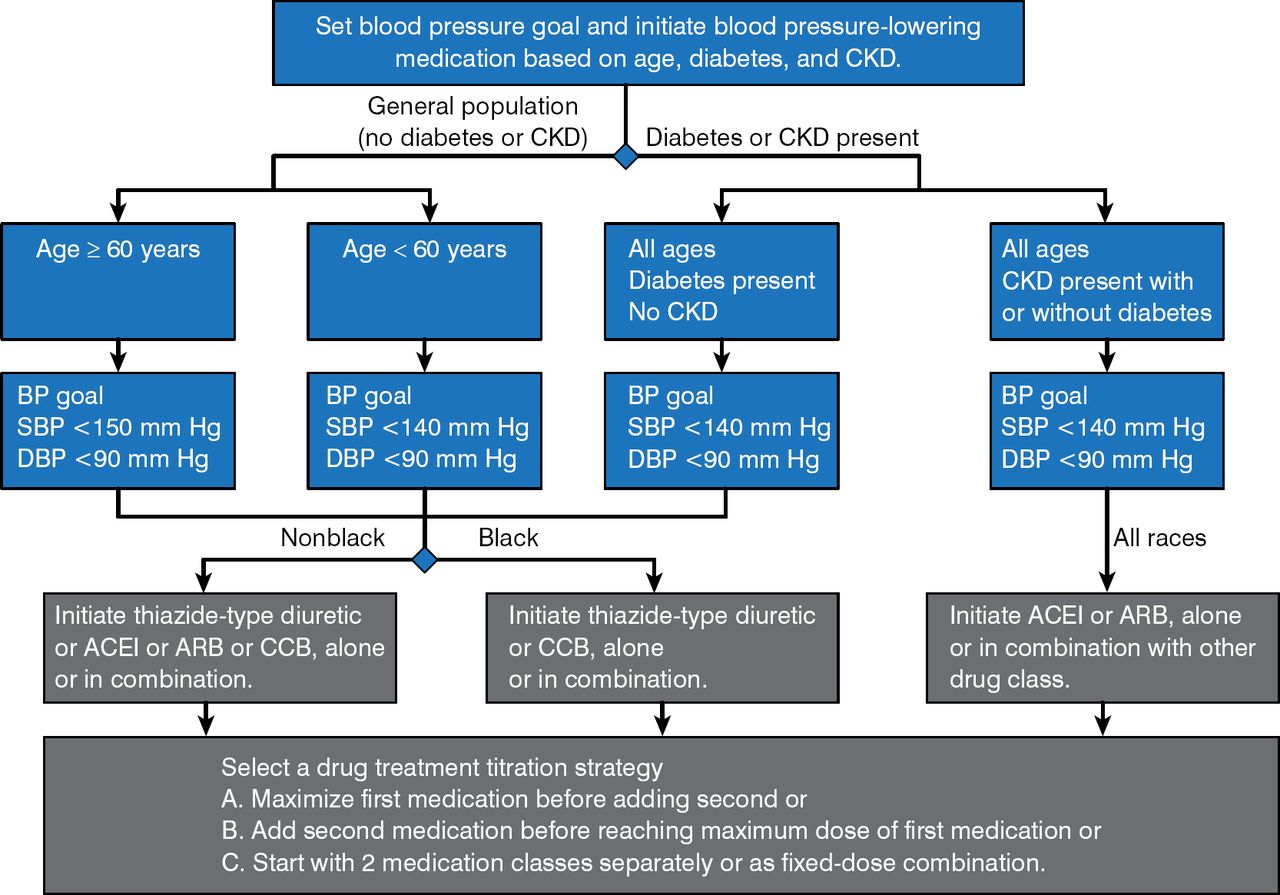
The JNC 8 algorithm for the management of high BP recommends initiating treatment with monotherapy and adding a second medication before reaching the maximum dose of the first antihypertensive (Figure 1).

JNC8 Algorithm for the Management of High BP in Adults
ACEI=angiotensin-converting enzyme inhibitor; ARB=angiotensin receptor blocker; BP=blood pressure; CCB=calcium channel blocker; CKD=chronic kidney disease; DBP=diastolic blood pressure; SBP=systolic blood pressure.
Reproduced from James PA et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. With permission from the American Medical Association.
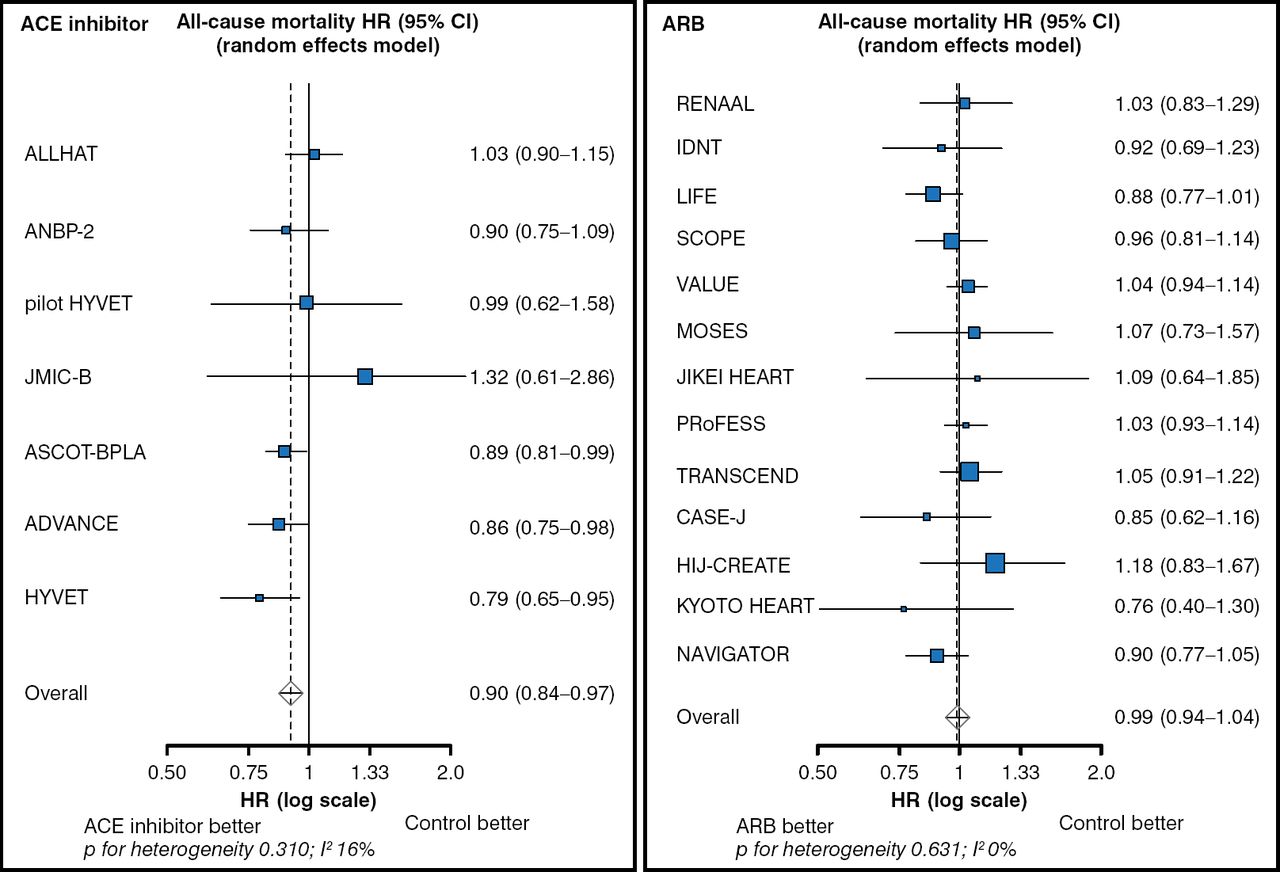
The ESH/ESC guidelines recommend any of the drug classes for monotherapy (Table 1) [Mancia G et al. Eur Heart J 2013]. This recommendation is supported by a meta-analysis on the use of antihypertensive drugs for preventing CVD [Law MR et al. BMJ 2009]. The most robust evidence supports using angiotensin-converting enzyme inhibitors (ACEIs), calcium channel blockers (CCBs), and nonthiazide diuretics for prevention of CVD and all-cause death. ACEIs have consistently been shown to prevent death from all causes, while angiotensin receptor blockers have demonstrated no all-cause mortality reduction and in some cases have been associated with an excess of mortality from myocardial infarction (Figure 2) [van Vark LC et al. Eur Heart J 2012; Strauss MH, Hall AS. Circulation 2006].
ESH/ESC Guidelines for Medical Management of HTN

Prevention of All-Cause Mortality: ACEIs and ARBs
ACEI=angiotensin-converting enzyme inhibitor; ARB=angiotensin receptor blocker.
Reproduced from van Vark LC et al. Angiotensin-converting enzyme inhibitors reduce mortality in hypertension: a meta-analysis of randomized clinical trials of renin-angiotensin-aldosterone system inhibitors involving 158 998 patients. Eur Heart J. 2012;33(16):2088–2097. With permission from Oxford University Press.
The ESH/ESC guidelines recommend adding second and third drugs when the BP target is not achieved. The use of fixed-combination therapy is supported [Gupta AK et al. Hypertension 2010], with emphasis on choosing a drug combination on the basis of trial success. ACEI—nonthiazide diuretics combinations (eg, indapamide and perindopril) and ACEI-CCB combinations (eg, benazepril and amlodipine) have been shown to prevent death from all causes [Jamerson K et al. N Engl J Med 2008; Patel A. Lancet 2007].
For elderly patients with systolic BP (SBP) ≥ 160 mm Hg, the ESH/ESC guidelines recommend reducing SBP to between 140 and 150 mm Hg. Antihypertensive treatment may be considered in fit elderly patients aged < 80 years with SBP ≥ 140 mm Hg if treatment is well tolerated.
Prof. Hall concluded that the HTN guidelines highlight the need for combination therapy, particularly with an ACEI plus a CCB. The evidence favors the ACEI perindopril, the CCB amlodipine, and the diuretic indapamide.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.