

Summary
Based on 2008 statistics, esophageal cancer is the eighth most common cancer worldwide, with nearly a half-million new cases each year and >400000 deaths. On the other hand, gastric cancer is currently not as prevalent in the United States as it was before, with an estimated 22220 cases and 10990 deaths in 2014, as US incidence has been declining steadily since the introduction of refrigeration. This article provides an overview of current approaches to the treatment of esophageal cancer, and reviews the epidemiology, biology, and patterns of failure for gastric cancer.
- Radiology
- Radiation Therapy
- Gastrointestinal Cancers
- Radiology
- Radiation Therapy
- Oncology
- Gastrointestinal Cancers
ESOPHAGEAL CANCER: CONTEMPORARY TREATMENT APPROACHES
Based on 2008 statistics, esophageal cancer is the eighth most common cancer worldwide, with nearly a half-million new cases each year and > 400 000 deaths [Jemal A et al. CA Cancer J Clin. 2011]. Whereas squamous cell carcinoma is predominant in Asia and East Africa, adenocarcinoma (ACA) is the prevalent form of the disease in Europe and North America. Ranking eighth for women, this cancer is the fifth most common in men with over twice the number of cases seen in women. If combined with gastric cancer, this disease category goes to number 3 for women and number 2 for men. There were nearly 18 000 new cases of esophageal cancer in 2013 and >15 000 deaths [Siegel R et al. CA Cancer J Clin. 2013]. Although 5-year survival has improved from 5% in the 1970s to 19% since 1999, the death rate in male patients increased by 7% from 1990 to 2007 [Devesa SS et al. Cancer. 1998].
Michael Haddock, MD, Mayo Clinic, Rochester, Minnesota, USA, provided an overview of current approaches to the treatment of esophageal cancer, drawing upon results from a number of relevant clinical trials. Moving from T1 patients, who potentially could be treated without surgery, to locally advanced disease, Dr Haddock outlined 3 options for T2 N0 patients (ie, surgery, chemoradiation, and trimodality therapy of chemoradiation plus surgery), but said that surgery alone is probably not a good option for this group. For T3 and T4 or node-positive patients, surgery alone is definitely not sufficient, and surgery needs to be accompanied by primary chemoradiation or trimodality therapy. For T4 patients, consideration should be given for radiation for palliation of dysphagia.
Providing historical perspective, results from RTOG 8501 [Hersokovic A et al. N Engl J Med. 1992], characterized as a landmark study first demonstrating that chemoradiation could be curative for esophageal cancer, were reviewed. However, severe to life-threatening toxicity occurred in 64% of the patients receiving the treatment regimen. Because cure rates for treatment involving surgery were low overall, the question regarding whether routine surgery following chemoradiation is indicated was addressed. Results from a German study [Stahl M et al. J Clin Oncol. 2005] in which patients were randomized to chemoradiation followed by surgery or no surgery showed no overall difference in survival, whereas patients receiving surgery were less likely to die of cancer but were more likely to die of treatment-related complications. A number of other studies were reviewed, none of which indicated a survival benefit for surgery alone (Table 1) [Pöttgen C, Stuschke M. Cancer Treat Rev. 2012].
Survival Rates at 4 Years Comparing Chemoradiation With and Without Surgery
An Australian meta-analysis exploring whether chemotherapy plus surgery was as effective as trimodality therapy was reviewed [Gebski V et al. Lancet Oncol. 2007]. The answer in a review of 19 clinical trials was that the addition of radiation therapy (RT) to chemotherapy conferred a statistically significant survival advantage (Table 2) [Sjoquist KM et al. Lancet Oncol. 2011]. An examination of pathologic complete response rates in several studies involving various chemoradiation therapy regimens led to a recommendation of 50-Gy RT with 2-drug chemotherapy.
Impact of Increasing Radiotherapy Dose on Pathologic Complete Response
In summary, Dr Haddock said that esophageal cancer is all too common and its incidence is increasing. Early stage disease can be treated with RT alone (ie, without surgery). Chemotherapy plus RT or trimodality therapy of chemoradiation and surgery is better than surgery alone, except in the treatment of T1b patients. Despite the many doses and regimens that have been used, RT with 50 Gy plus 2-drug chemotherapy should be considered standard. Reinforcing the importance of RT in treatment of esophageal cancer, Dr Haddock reminded the audience that the relapse rate in the radiation fields in a recent study on the CROSS trials [Oppendijk V et al. J Clin Oncol. 2014] was only 5%, and that relief was experienced by approximately 80% of patients receiving RT as palliative therapy for dysphagia.
GASTRIC CANCER: CONTEMPORARY TREATMENT APPROACHES
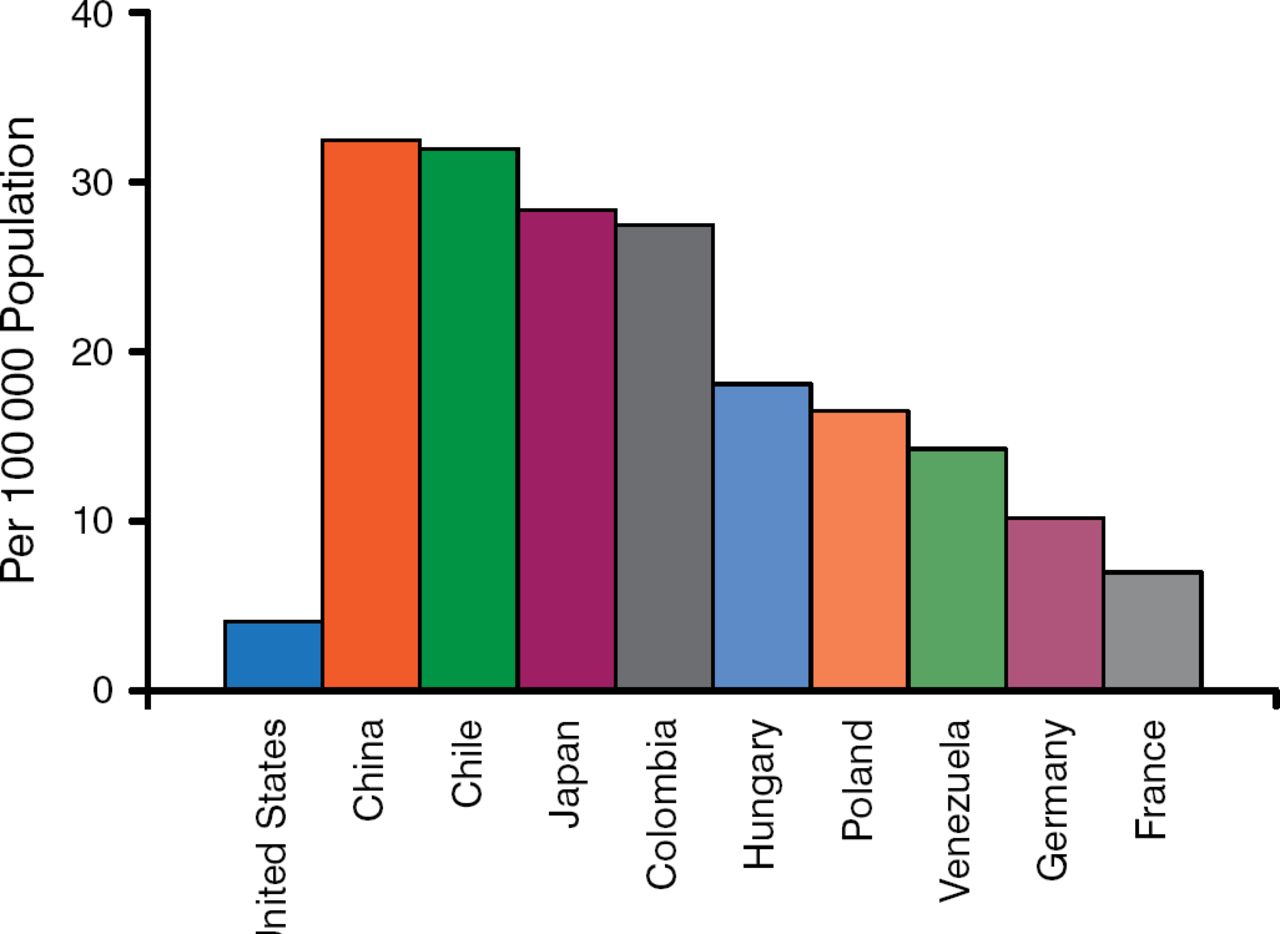
Gastric cancer is currently not as prevalent in the United States as it was before, with an estimated 22 220 cases and 10 990 deaths in 2014, as US incidence has been declining steadily since the introduction of refrigeration [Ferlay J et al. Int J Cancer. 2010]. However, gastric cancer is the second leading cause of cancer death worldwide, with 1 million new cases and > 700 000 deaths per year, with over one-half of these cases occurring in East Asia, particularly Korea and Japan (Figure 1).

Regional Variation in Gastric Cancer Mortality
Reproduced with permission from HJ Mamon, MD, PhD.
Harvey J. Mamon, MD, PhD, Brigham and Women's Hospital, Boston, Massachusetts, USA, delivered a talk that reviewed the epidemiology, biology, and patterns of failure for gastric cancer, focusing on the role of radiation in a multidisciplinary approach to treating gastric ACA. Results of recently completed clinical trials as well as selected ongoing trials were reviewed.
Risks for gastric cancer include nutritional factors such as salted meats or fish and high nitrate consumption. Prior gastric surgery and Helicobacter pylori infection are also risk factors, as well as lack of refrigeration, smoking, and low social class. The Lauren classification, now nearly 50 years old, differentiates tumors as either intestinal (well-differentiated glandular formations with intact intercellular adhesion molecules) or diffuse (poorly differentiated, less structured, and more invasive, with defective intercellular adhesion molecules). The World Health Organization classification of 4 sub-types (papillary, tubular, mucinous, and poorly cohesive) is used less frequently than the Lauren classification. Neither is sufficient to guide disease management effectively in terms of prognostic or predictive information. However, The Cancer Genome Atlas project offers hope of a more useful classification based on molecular characteristics of gastric tumors with information derived from copy number, RNA sequencing, DNA methylation patterns, and microsatellite instability, with 4 subgroups already identified. One of the four molecular subgroups of gastric tumors, the “Epstein-Barr virus subtype,” displays the highest prevalence of DNA hypermethylation in any cancer studied to date.
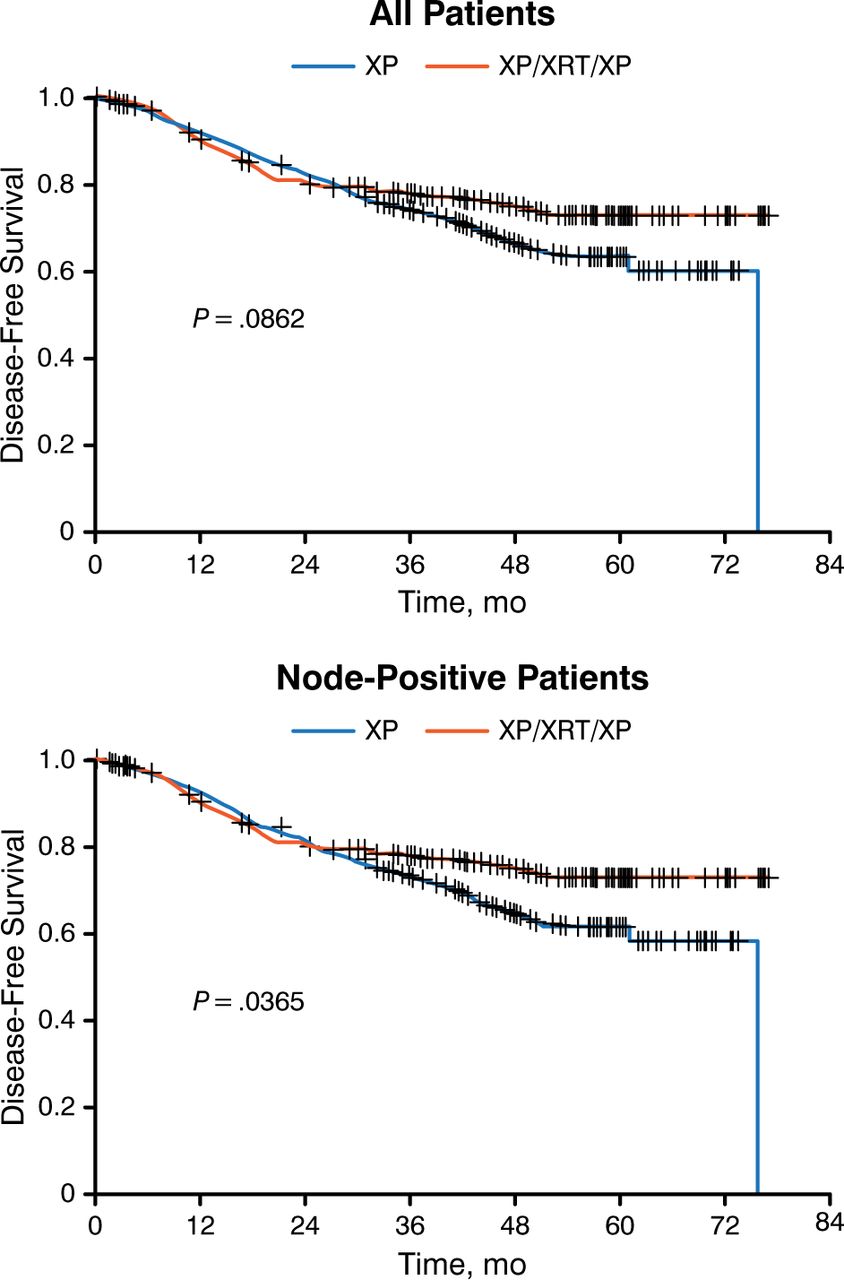
Several clinical trials comparing surgery alone to surgery plus chemotherapy or chemotherapy plus RT were covered, the upshot being that surgery alone resulted in lower overall survival (OS) rates. In terms of trials covering the addition of RT to protocols with both surgery and chemotherapy, ARTIST [Lee J et al. J Clin Oncol. 2012] was a South Korean study of 458 patients randomized to postoperative chemotherapy or chemotherapy with RT (Figure 2). Only disease-free survival (DFS) was reported due to fewer deaths than expected, precluding an analysis of OS. Multivariate analysis indicated that the addition of radiation significantly prolonged DFS (HR, 0.687; 95% CI, 0.474 to 0.995; P = .047).

Disease-Free Survival in the ARTIST Trial
Lee J et al. J Clin Oncol. 2012;30:268–273. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
One notable meta-analysis included 5 randomized studies comparing adjuvant chemotherapy with adjuvant chemoradiation [Ohri N. Int J Radiat Oncol Biol Phys. 2013]. Adjuvant radiation was associated with an approximately 20% improvement in OS and DFS in all subgroups analyzed.
Dr Mamon concluded by reminding the audience that although incidence is declining in Europe and North America, gastric cancer remains a major problem worldwide with surgery remaining as the primary curative therapy. While multiple studies suggest that adjuvant and neoadjuvant chemotherapy and RT can have benefit, much is still to be learned about how to best select patients for various treatment combinations and their optimal sequencing. A deeper understanding of the underlying molecular mechanisms of gastric cancer should lead to greater detail in the classification of tumors, enabling physicians to make more informed choices in therapy selection.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.