

Summary
For patients to gain maximal benefit from bariatric surgery, it is important for them to receive effective postoperative care through recognition of physiological and medical changes, effective behavioral interventions, ways to promote physical activity, and requirements for nutritional supplementation.
- Obesity
- Deficiency Disorders
- Obesity
- Deficiency Disorders
- Endocrinology
- Diabetes & Metabolic Syndrome
For patients to gain maximal benefit from bariatric surgery, it is important for them to receive effective postoperative care through recognition of physiological and medical changes, effective behavioral interventions, ways to promote physical activity, and requirements for nutritional supplementation.
Dmitry Nepomnayshy, MD, Lahey Hospital and Medical Center, Burlington, Massachusetts, USA, gave a presentation that explained important considerations in managing comorbidities of obese patients postoperatively, which conditions improve following surgery and which do not, and methods to handle new conditions that arise following surgery.
Although bariatric surgery leads to improvements in medical problems, some of these problems such as diabetes may return later. After surgery, a variety of individuals including the surgeon, bariatrician, endocrinologist, family practitioner, other medical practitioners, therapist, family, and friends all need to work together to provide care in the hospital and then at home.
For example, diabetes often goes away following bypass, but has a tendency to return [Brethauer SA et al. Ann Surg. 2013]. In the hospital, oral medications should be withheld, blood glucose should be monitored frequently (target range, 90–150 mg/dL), insulin may need to be restarted, and an endocrinology consultation is recommended. At home, metformin (if previously prescribed) may be restarted once the patient can take oral medication. However, other oral medications are not usually recommended. It is important to carefully watch for dehydration and hypoglycemia; blood glucose should be monitored even in the absence of medication. If the diabetes appears to be in remission, monitoring should be continued because of the risk of recurrence. Education of the patient and family is important to aid in monitoring.
There is an approximately 40% reduction in cardiac risk following surgery [Romeo S. Diabetes Care. 2012]. Like blood glucose, blood pressure should be carefully monitored. When weaning patients from medications, it is recommended that medications with the greatest side effects be weaned first. Angiotensin-converting enzyme inhibitor and angiotensin receptor blocker use should be maintained at first, but patients may later be weaned from these if careful monitoring for arrhythmias is used. Hypotension can occur in patients who are using these medications at the time of surgery, so it may be advisable to discontinue them prior to surgery. Trial and error may be needed, managed by the cardiologist or primary care physician. Liver disorders including nonalcoholic steatohepatitis (NASH) also improve, especially in the first year [Mathurin P et al. Gastroenterology. 2011]. This is closely linked to insulin resistance, and liver disorders may become worse if diabetes recurs. Progression from hepatitis to cirrhosis may be silent; a liver biopsy, repeated a year later, may be sufficient unless a patient's diabetes returns or NASH does not go away.
Lipid disorders also improve following surgery, with decreases in triglycerides accompanied by increases in high-density lipoprotein cholesterol [Suter M et al. Ann Surgery. 2011]. These results tend to be sustained and medication may be weaned with careful monitoring. However, some patients may continue to have lipid disorders requiring therapy despite weight loss.
Respiratory medication use decreases by about 50% following surgery [Sikka N et al. Ann Allergy Asthma Immunol. 2010]. However, clinicians should be aware that patients sometimes stop using CPAP machines as they feel better while they may still have sleep apnea. It is important to carefully document whether patients continue to have apnea regardless of whether they feel better.
Complications include micronutrient deficiencies [Gudzone KA et al. Obes Surg. 2013], reflux, abdominal pain, and hypoglycemia. Bone density should be checked annually. Patients may also regain weight, but the causes of this are not fully understood. It could be due to adaptation to their new physiology/anatomy, behavioral factors, and genetics. To prevent regain, long-term follow-up is needed, support and medication may be needed, and additional surgery may sometimes be required. Antidepressant use [Cunningham JL et al. Obes Surg. 2012] and substance abuse disorders do not appear to improve following surgery [Raebel MA et al. JAMA. 2013].
To ensure the best outcomes, patients need coordinated, long-term care with careful monitoring by a health care team and education about possible medical changes following surgery.
Paul Davidson, PhD, Brigham and Women's Hospital, Boston, Massachusetts, USA, specifically addressed postoperative behavioral health concerns and initial behavioral involvement.
A psychological/psychiatric assessment is important prior to surgery to evaluate each patient's needs, but the assessment is intended to help patients prepare rather than to act as a barrier to surgery. This type of evaluation may help to determine timing, to address anxiety, and to improve patient education while identifying individuals who may be poor candidates for surgery. Additionally, the presurgical evaluation can help to motivate the patient to make the necessary changes to improve his or her health while developing a therapeutic alliance that can be helpful post surgically.
Organizational guidelines are generally focused on preoperative behavioral involvement, but there is a need for postoperative involvement as well for all patients. Dr Davidson presented examples of primary literature supporting the case that patients offered postoperative counseling were more motivated to follow up and to participate in counseling than those given preoperative counseling [Kalarchian MA et al. Surg Obes Relat Dis. 2012; Lier HØ et al. Patient Educ Couns. 2012; Leahey TM et al. Surg Obes Relat Dis. 2009]; additionally, there is evidence that weight loss is greater in patients who attend support groups postoperatively [Orth WS et al. Obes Surg. 2008]. A review and meta-analysis found greater weight loss in patients given postoperative behavioral care [Rudolph A, Hilbert A. Obes Rev. 2013].
Problematic eating behavior can lead to postoperative behavior referrals. For example, patients may demonstrate mindless eating, binge eating, and bulimia following surgery [Neff KJ, le Roux CW. J Clin Pathol. 2013; Marcus MD et al. Am J Psychiatry. 2009]. Patients have less depression, but more anxiety, and some are disappointed that weight loss does not fix more problems in their lives. Suicide risk increases about 2 years following surgery. There is also an increased risk of alcohol abuse, drug abuse, smoking, gambling, and shoplifting. In particular, weight gain can be associated with feelings of failure and with negative effects on quality of life [Karlsson J et al. Int J Obes (Lond). 2007].
Patients may show a lack of compliance following surgery, including resistance to recommendations. Patients may also have difficulty adjusting to their physical changes. Relational concerns can also emerge and there is a risk of breakup or divorce; it is important to address concerns regarding sexuality as well. It may take several years for some of these issues to emerge and patients may minimize concerns, so it is important for the health care team to recognize the need for behavioral interventions.
Some emotional and psychological issues improve following surgery, but many complex issues remain or can develop postoperatively. There is some limited evidence that patients may be more receptive to behavioral intervention postoperatively and that postoperative behavioral care has multiple benefits, including greater weight loss.
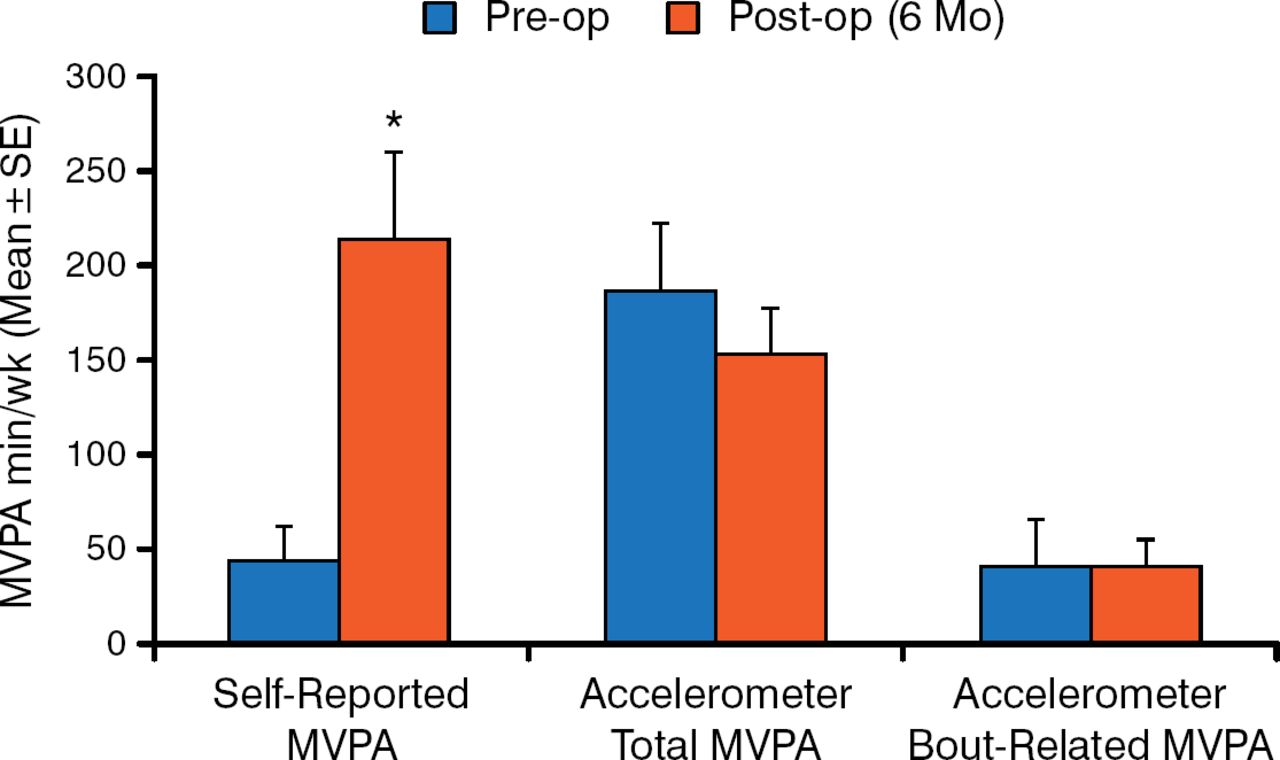
Dale Bond, PhD, Brown University, Providence, Rhode Island, USA, addressed guidelines regarding physical activity. Physical activity can improve physical and mental quality of life in multiple ways, for example, improved physical function, bodily pain, energy, and mental and social health. Preoperative physical activity is a strong predictor of postoperative physical activity and may also be important perioperatively in the form of reduced operative time, complications, and rate of recovery. Postoperatively, increased physical activity is associated with increased weight loss and better glucose control. However, a challenge to improving physical activity is that bariatric surgery patients tend to be both inactive and highly sedentary preoperatively and make only modest changes in these behaviors postoperatively. [Bond DS et al. Surg Obes Rel Dis. 2010; Bond DS et al. Obes Surg. 2011]. Although patients report substantial increases in activity (as high as 500%) following surgery based upon questionnaires, objective measures do not support these increases (Figure 1) [Bond DS et al. Obesity (Silver Spring). 2010].

Moderate to Vigorous Physical Activity Preoperatively vs 6 Months Postoperatively
MVPA, moderate to vigorous physical activity; SE, standard error.
*P = .004.
Adapted from Bond DS et al. Pre- to postoperative physical activity changes in bariatric surgery patients: self report vs objective measures. Obesity. 2012;18:2395–2397. Copyright © 2012 The Obesity Society.
Research indicating that many patients either do not change or make only modest changes in their physical activity postoperatively supports the American Association of Clinical Endocrinologists/The Obesity Society/American Society for Metabolic and Bariatric Surgery (AACE/TOS/ASMBS) guideline statement that negative beliefs and cognitions with respect to physical activity must also be addressed to improve activity levels. However, this statement does not provide specific, evidence-based guidelines to address the issue with patients.
The American College of Sports Medicine and ASMBS have developed guidelines to collaborate on a systematic review to publish a position paper to address this issue. As a first step, 7 critical questions have been developed. For example, the collaborators intend to examine whether patients increase physical activity following surgery, whether activity before surgery predicts activity following surgery, and whether activity prior to surgery predicts weight loss following surgery. The collaborators will examine the literature for answers to these questions and use National Institutes of Health Heart, Lung, and Blood Institute criteria to grade the quality of the evidence before publishing their position paper.
Lynn Bolduc, MS, RD, Eastern Maine Medical Center, Bangor, Maine, USA, addressed the 2013 AACE/TOS/ ASMBS guidelines for the use of vitamins and minerals. Nutrient deficiencies are common following bariatric surgery, but deficiencies are also common in these patients prior to surgery. The requirements for postoperative assessment of nutritional state vary depending on the procedure but should include such tests as protein/albumin, iron, B12, and 24-hour urinary calcium with additional analyses for some procedures. Supplementation recommendations vary based on the procedure, but may be empiric as screening can be costly. Calcium (as calcium citrate or in the diet), vitamin D, and a multivitamin with folic acid and thymine (and iron if not supplemented separately) are recommended. Vitamin D levels vary by season and ideally should be measured at different times of the year. There is insufficient evidence to recommend screening for essential fatty acids, vitamin E, and vitamin K at this time, although vitamin K levels should be checked if there are deficiencies in other fat-soluble vitamins. However, screening for vitamin A is recommended for biliopancreatic diversion and biliopancreatic diversion with duodenal switch. All patients should be monitored for anemia, and patients with anemia should be tested for other deficiencies as well.
After presenting detailed recommendations for screening and monitoring, Prof Bolduc concluded by emphasizing that the clinical practice guidelines are designed to help in decision making based upon the current state of evidence-based knowledge and that the release of the 2014 ASMBS Nutrition Guidelines may result in updated clinical practice guidelines as well.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.