

Summary
lthough people are often successful in losing weight, sustaining weight loss and healthy eating over the long term is challenging for many. New behavioral strategies can be used to help patients use acceptance and mindfulness to improve decision making. Additionally, behavioral strategies can help to promote a healthy environment for children, reducing the risk of obesity and related medical complications.
- Obesity
- Nutrition Physiology
- Prevention & Screening
- Obesity
- Nutrition Physiology
- Endocrinology
- Diabetes & Metabolic Syndrome
- Prevention & Screening
Although people are often successful in losing weight, sustaining weight loss and healthy eating over the long term is challenging for many. New behavioral strategies can be used to help patients use acceptance and mindfulness to improve decision making. Additionally, behavioral strategies can help to promote a healthy environment for children, reducing the risk of obesity and related medical complications.
Evan Forman, PhD, Drexel University, Philadelphia, Pennsylvania, USA, explained ways that internal factors (such as motivation) and external factors (such as the availability of unhealthy food) contribute to behavior and cause difficulty in weight maintenance even though behavioral changes often allow successful weight loss initially. Over time, commitment can erode because of reduced reinforcement (eg, as weight loss slows), biological and environmental pressures, and the effort required to refrain from consuming unhealthy food that is readily available in the environment. Unhealthy choices can result from an attempt to escape from uncomfortable states (eg, anxiety, hunger, and boredom) and to seek pleasure. By addressing factors that patients can change, promoting mindfulness, and helping them to accept internal discomfort, it may be possible to improve their ability to sustain healthier behavior choices.
Dr Forman summarized the framework of acceptance-based therapy (ABT) by explaining that patients can change some things and learn to accept others using certain skills that can be developed. For example, patients can plan meals, purchase healthy foods, eat regularly, exercise, and reduce portion sizes. However, they cannot avoid difficult internal experiences (such as anxiety and urges to eat) or environmental factors (such as images and the presence of unhealthy food in some locations). To cope, they can learn nutritional, behavioral, and environmental skills while improving their ability to tolerate distress, develop a mindful awareness of their own decision making and values, and make a commitment to healthy behaviors. Of particular importance to sustain weight loss, patients must learn how to experience cravings and internal discomfort without overeating, to be aware of their decisions, and to cope well with lapses.
ABT has 5 treatment targets (acceptance, willingness, defusion, mindfulness, and values clarification). Defusion refers to the ability to separate thoughts and feelings from actions. Patients learn to accept their feelings, to experience urges without acting, to be mindful while making deliberate choices, to address problematic thoughts, and to be aware of their own values. The components unique to ABT (compared with standard behavioral therapy [SBT]) are clarification of values, mindfulness training, and acceptance of difficult internal states.
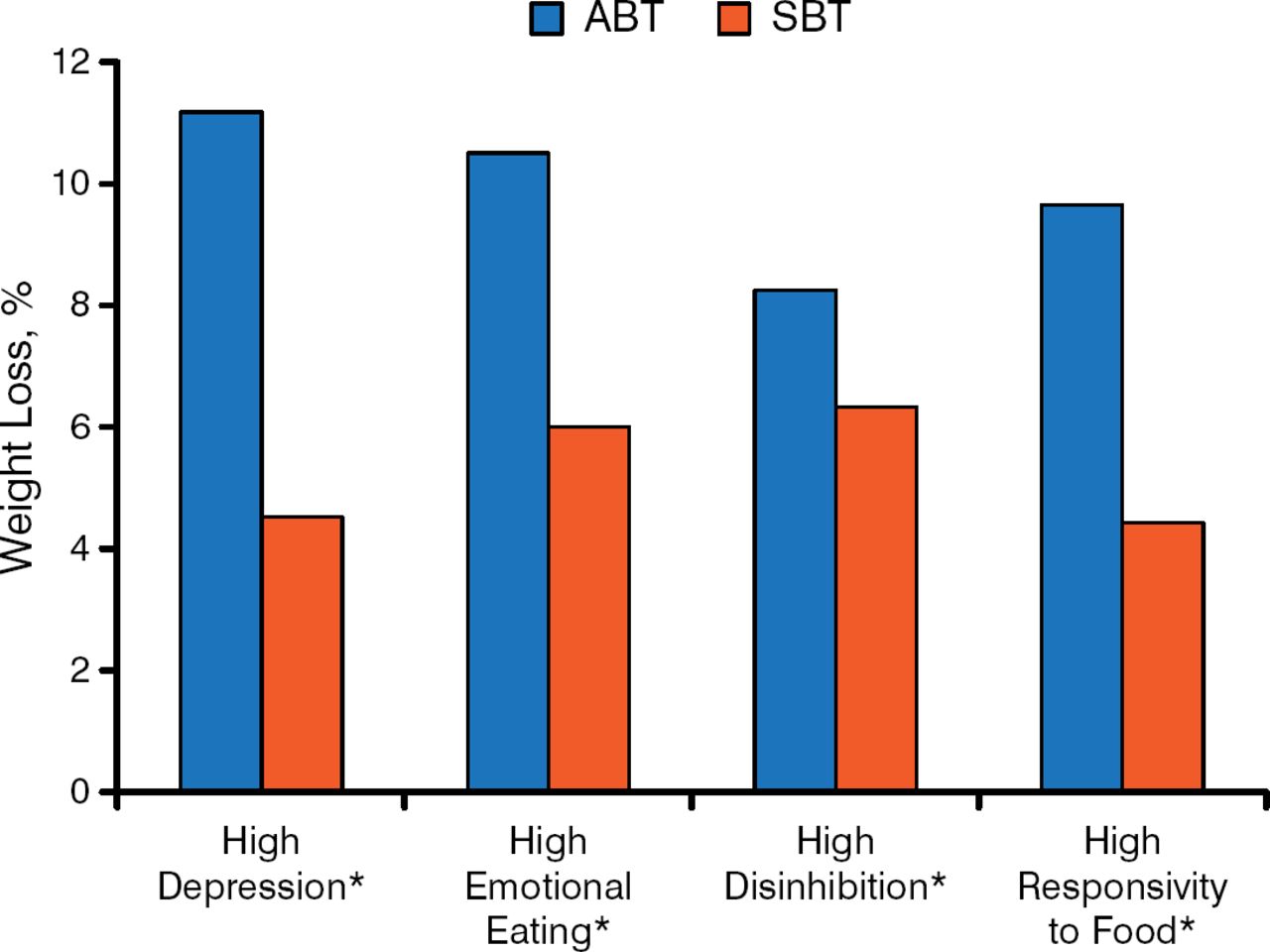
Dr Forman presented the results from several studies that provide empirical evidence that ABT can be effective, especially for patients with high disinhibition, more discounting of long-term rewards, or other risk factors. One study demonstrated that cravings were lower in patients treated with ABT vs cognitive behavioral therapy (CBT) [Forman EM et al. Behav Res Ther. 2007]. Additionally, patients who were the most susceptible to eating cues showed the greatest benefit in the Mind Your Health study, which examined patients treated with ABT vs SBT (Figure 1) [Forman EM et al. Obesity (Silver Spring). 2013]. Early treatment nonresponders showed a greater benefit of ABT in the preliminary results from the Mind Your Health II study. ABT teaches skills that help people make better decisions even when faced with internal and external challenges.

Weight Loss With SBT and ABT Moderated by Susceptibility
ABT, acceptance-based therapy; SBT, standard behavioral therapy.
*P < .05.
Adapted from Forman EM et al. The Mind Your Health project: A randomized controlled trial of an innovative behavioral treatment for obesity. Obesity. 2013;21:1119–1126. Copyright © 2013 The Obesity Society.
MINDFULNESS WHEN EATING
Jean L. Kristeller, PhD, Indiana State University, Terre Haute, Indiana, USA, presented components of Mindfulness-Based Eating Awareness Training (MB-EAT) and discussed results of several studies examining its effectiveness. She emphasized that mindfulness makes a difference because it allows people to pause to consider automatic reactions, allowing them to use higher-level thought for decision making. As Dr Forman also emphasized, this type of approach provides skills that can be used to maintain weight loss. Dr Kristeller noted that patients are used to high-calorie diets and very restrictive diets, but often do not know how to maintain a flexible, healthy diet that is intermediate between those extremes.
MB-EAT involves consideration of the knowledge about nutrition and exercise combined with research into food intake regulation, weight loss (including CBT approaches), disordered eating, and hunger and satiety regulation. Dr Kristeller explained the 3 stages of mindfulness meditation (heightened awareness, reduced automatic reactivity, and emergence of appropriate self-care and response) [Kristeller JL. Mindfulness meditation. In: Lehrer P et al. Principles and Practice of Stress Management. New York: Guilford; 2007]. She then discussed the skills that can be developed in MB-EAT, including the ability to recognize responses to food and heightening interoceptive awareness of physical hunger and satiety cues, both taste satiety and fullness. By paying attention to taste satisfaction, patients can consider whether it is worth continuing to eat as the satisfaction level decreases. Additionally, patients develop awareness, acceptance, and a better attitude toward eating and food.
Dr Kristeller continued by reviewing empirical support for mindfulness-based approaches. Studies included patients with binge-eating disorders and over-eaters, as populations have different eating patterns that must be considered. The first trial [NCT00032760] found obese individuals with binge eating disorder had significant improvement, equivalent to a CBT-based program, in decrease in binge eating, and greater improvement overall in a sense of control around eating. Increased engagement in mindfulness and meditation correlates with overall improvement and greater weight loss [Kristeller JL et al. Mindfulness. 2012]. Dr Kristeller said that in another trial currently under review, these positive benefits were shown to be similar for those with or without BED, and with moderate to morbid obesity. The unpublished SHINE study [NCT00960414] comparing a treatment group undergoing mindfulness treatment (MB-EAT, exercise, and stress reduction) with a control group (receiving nutrition information and exercise) found a greater percentage of weight loss, a decrease in fasting glucose levels, and a decrease in triglycerides/HDL level in the mindfulness group.
CHILDHOOD OBESITY RISK FACTORS
Melinda S. Sothern, PhD, Louisiana State University Health Sciences Center, New Orleans, Louisiana, USA, addressed modifiable risk factors for obesity in children and barriers to having a healthy weight, strategies to improve nutrition and physical activity to modify risk for obesity, and solutions to some of the potential barriers.
Modifiable risk factors for childhood obesity are numerous, including poor family role modeling, use of sugary beverages, large portion sizes, use of food as a reward, excessive media time, and lack of opportunities for outdoor play. Dr Sothern provided information for addressing a range of these risk factors. For example, parents can improve their own food choices, improve family sleep habits, increase the frequency of family meals, decrease snacking, and provide water (between meals) or milk (for mealtimes) instead of sugar-sweetened beverages among other practices [Pan L et al. Pediatrics. 2014; Anderson SE, Whitaker RC. Pediatrics. 2010; O'Connor TM et al. Pediatrics. 2006]. Praising children for physical activity and serving a healthy breakfast are also helpful approaches [O'Dea JA, Wilson R. Health Educ Res. 2006; Alexander KE et al. Obesity (Silver Spring). 2009].
Because children may resist healthy food, Dr Sothern suggests gradually replacing non-nutritious foods with better options and making nutritious food easily accessible in the home (within reach of children). She also noted that children should be encouraged to leave food on their plates when finished, allowing them to choose to eat the right amount for their appetite [Spruijt-Metz D et al. Am J Clin Nutr. 2002; Entin A et al. J Am Coll Nutr. 2014]. Additionally, children should not be taught to label foods as good or bad or given food as a reward.
In addition to giving detailed recommendations for multiple risk factors and barriers, Dr Sothern emphasized that children have different needs than adults. For example, they have immature metabolic systems, need movement and play, cannot focus for long time periods, and have lower oxygen uptake [Sothern M. Profile of the Overweight Child. In: Safe and Effective Exercise for Overweight Youth. Boca Raton, FL: CRC Press; 2014]. These factors need to be considered in making recommendations to improve their health.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.