

Summary
This article discusses 2 recently published studies that provide insight into relatively new dermatologic conditions, as well as new therapeutic approaches to treating skin disease.
- Skin Diseases
- Dermatology
- Skin Diseases
- Exclusive Article - For home page
Rick Hoekzema, MD, PhD, Free University and Academic Medical Center, Amsterdam, The Netherlands, discussed 2 recently published studies that provide insight into relatively new dermatologic conditions. The first was a retrospective study of a series of patients with clinical features of urticarial dermatitis (UD) [Hannon GR et al. J Am Acad Dermatol. 2014]. The second study discussed cutaneous side effects seen in patients treated with V-raf murine sarcoma viral oncogene homolog B1 (BRAF) inhibitors [Vanneste L et al. J Eur Acad Dermatol Venereol. 2014]. Prof Hoekzema focused on the ramifications of these findings, particularly the need for careful monitoring of patients following BRAF inhibitor treatment.
In a 2006 article, Kossard and colleagues [Arch Dermatol. 2006] reported that patients presenting with urticarial plaques and papules had features resembling urticaria; however, the individual lesions lasted > 24 hours and often for days. Kossard et al. concluded that UD “seems to be a useful histological and clinical term for a subset of the dermal hypersensitivity reaction pattern.”
Prof Hoekzema also further discussed the retrospective 6-year review of clinical and laboratory evaluations (including histology), as well as the final diagnosis and associations for 146 patients with clinical features of UD who were seen at the Mayo Clinic during 2006 through 2012 [Hannon GR et al. J Am Acad Dermatol. 2014]. UD was confirmed in 70 patients, 40 of whom also had histopathologic results concordant with Kossard's description of UD. Of these 40 patients, 10% had a history of malignancy within 4 months of UD onset, prompting the investigators to question whether UD can be paraneoplastic and whether there is a need for malignancy screening in recalcitrant cases. The investigators concluded that UD is characterized by both urticarial and eczematous lesions, and patients with UD can have an array of diagnoses including various subtypes of dermatitis, drug eruptions, bullous pemphigoid, and scabies.
Prof Hoekzema believes UD does not represent a disease entity but a reaction pattern, both clinically and histologically. Although idiopathic UD may exist, he sees it as a diagnosis of exclusion for which underlying common causes such as medication reaction and pemphigoid need to be excluded first.
BRAF inhibitors prolong survival in patients with BRAFV600E-positive metastatic melanoma by 3 to 4 months by way of a disruption in the mitogen-activated protein kinase (MAPK) signaling pathway [Chapman PB et al. N Engl J Med. 2011]. Growth factors that bind to the receptor tyrosine kinase activate the MAPK pathway. Overactivation of the transcription factor associated with this pathway stimulates cell growth that can lead to cancer development in keratinocytes. BRAF inhibitors prevent overactivation and proliferation in malignant cells. However, the cause of epidermal proliferation (including squamous cell carcinomas, keratoacanthomas, and verrucous keratoses) is a paradox that is not fully understood. Although he did not discuss this paradox in detail, Prof Hoekzema suggested a recent review by Holderfield and colleagues [Br J Cancer. 2014] as further reading.
In a second study, Vanneste and colleagues [J Eur Acad Dermatol Venereol. 2014] reported the significant cutaneous adverse events (AEs) associated with BRAFV600E treatment when used to treat patients with a BRAF mutant (V600E, V600K, V600R) metastatic melanoma. Of the 20 patients treated with BRAF inhibitors, 11 (58%) developed cutaneous side effects and 10 (42%) had > 1 cutaneous AE. The major side effect was verrucous papillomas observed in 8 (42%) patients after 1 to 12 weeks. Other effects are shown in Table 1.
Prevalence and Timing of Cutaneous Side Effects Following BRAF Treatment
Patient education (especially the need for photoprotection) and early identification and management can minimize these AEs and allow the patient to continue BRAF treatment without interruption and often without dose reduction. These patients should be treated by a team that includes a dermatologist; close and consistent cutaneous follow-up may be required. In those patients with unmanageable cutaneous AEs, combination therapy with a mitogen-activated protein kinase kinase (MAP2K) inhibitor helps decrease the incidence. Thus, the use of other inhibitors of the MAPK cascade or inhibition of other signaling pathways may be helpful in the management of these toxicities.
Hok Bing Thio, MD, PhD, The Erasmus University Medical Center, Rotterdam, The Netherlands, surveyed a series of new therapeutic approaches to treating skin disease.
After 15 years of innovations in gene therapy, only 1 patient with an inherited skin disorder has been successfully treated in a clinical trial [Abdul-Wahab A et al. Semin Cutan Med Surg. 2014]. Prof Thio attributed this to the fact that multiple genes are often involved in skin disorders.
Immunotherapeutics have been very successful in benign and malignant skin diseases [O'Shea JJ et al. Cell. 2014]. For instance, inhibition of interleukin (IL)-17A, implicated in the pathogenesis of autoimmune disorders, reduces psoriasis symptoms [Patel DD et al. Ann Rheum Dis. 2013]. Besides psoriasis and psoriatic arthritis (PsA), IL-17 is implicated in rheumatoid arthritis and Behçet disease. Five biological drugs for silencing psoriasis are in clinical use and more are in the pipeline [Crow JM. Nature. 2012].
Apremilast is a small molecule that modulates the production of proinflammatory and anti-inflammatory mediators and inhibits the intracellular signal transducing protein phosphodiesterase-4 [Schafer PH et al. Cell Signal. 2014; McCann FE et al. Arthritis Res Ther. 2010; Schett G et al. Ther Adv Musculoskelet Dis. 2010]. Apremilast appears to be a potential new agent for the treatment of both rheumatoid arthritis and PsA.
There are already a variety of established immunomodulatory therapies for patients with multiple sclerosis (MS) and several new treatments are in or have recently completed clinical trials [Cross AH, Naismith RT. J Intern Med. 2014]. Although many of these therapies have potential in the treatment of dermatologic conditions, at least 1 treatment for MS (dimethylfumarate) has emerged from the successful treatment of psoriasis.
In one study, more complete suppression of immunoglobulin E (IgE) with ligelizumab, a novel high-affinity humanized monoclonal IgG1κ anti-IgE, proved superior to omalizumab in suppressing skin-prick wheal responses to an allergen [Arm JP et al. Clin Exp Allergy. 2014].
KIT, BRAF, MAP2K, and extracellular signal-regulated kinase inhibitors that block mutations in the MAPK pathway are proving effective in the treatment of metastatic melanoma. Such mutations lead to oncogenic cell proliferation and loss of apoptosis function. The anti-cytotoxic T lymphocyte A4 antibody, ipilimumab, which prevents downregulation of the immune system, can lead to significant increases in survival for patients with metastatic melanoma, whereas nivolumab, a fully human IgG4 monoclonal antibody, blocks ligand activation of PD-1, a protein called programmed cell death that is important for apoptosis [Ledford H. Nature. 2014 (vol 7494)].
Epigenetic mutations in basal keratinocytes in the epidermis caused by the sun may promote hyperproliferative precancerous keratinocytes. Topical applications of agents such as 5-fluorouracil, imiquimod, and ingenol mebutate are used with success to treat superficial skin cancer, primarily actinic keratosis and basal cell carcinomas [Micali G et al. J Am Acad Dermatol. 2014].
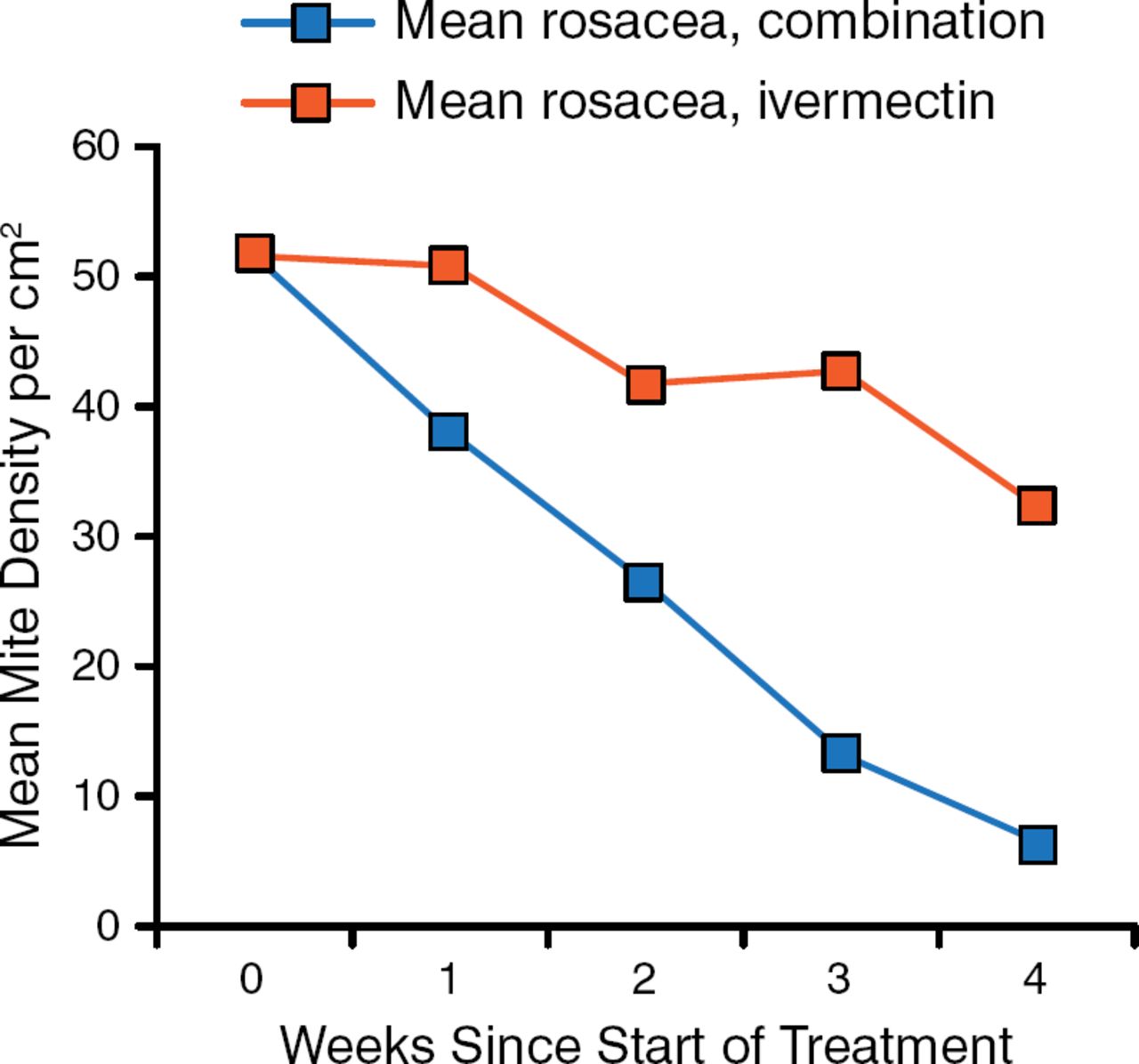
Prof Thio went on to discuss other agents with the potential to treat dermatologic conditions. Brimonidine, a highly selective α2-adrenerigc agonist, reduces erythema of rosacea through direct cutaneous vasoconstriction [Fowler J et al. J Eur Acad Dermatol Venereol. 2014]. Demodex folliculorum is the most common human ectoparasite. Because rosacea is linked to the presence of this parasite, it can be treated with ivermectin, especially when combined with metronidazole (Figure 1) [Salem DA. Int J Infect Dis. 2013].

Comparison of Invermectin and Invermectin Plus Metronidazole on Mite Density
Combination treatment comprises invermectin plus metronidazole.
Adapted from International Journal of Infectious Diseases, 17:e343–e347. Salem DA et al, Evaluation of the efficacy of oral ivermectin in comparison with ivermectin-metronidazole combined therapy in the treatment of ocular and skin lesions of Demodex folliculorum, Copyright 2013, with permission from International Society for Infectious Diseases.
According to Prof Thio, the role of gastrointestinal and cutaneous microbiota in healthy skin and in inflammatory and allergic skin diseases is also an area of scientific interest [Maccaferri S et al. Dig Dis. 2011]. As an example, he highlighted a study showing that consuming a candy that contained 2.1% kimchi-derived Lactobacillus plantarum K8 cell lysate can improve skin barrier function and repair [Kim H et al. J Microbiol Biotechnol. 2014].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.