

Summary
In the United States, 32% of children are considered overweight, and 16% are obese. Recent trends show a slowing increase in this prevalence. However, 5% of the nation's youth are considered severely obese, a trend that continues to increase among those aged 6 to 19 years [Ogden CL et al. JAMA 2010]. Aside from the psychological and physical issues associated with pediatric and adolescent obesity, the condition also increases the risk of problems later in life, including type 2 diabetes mellitus, asthma, end-stage renal disease, obstructive sleep apnea, and severe ambulatory limitations [Inge TH et al. Pediatrics 2013].
- Obesity
- Pediatric Nutrition
- Prevention & Screening
- Obesity
- Pediatric Nutrition
- Prevention & Screening
- Endocrinology
- Diabetes & Metabolic Syndrome
In the United States, 32% of children are considered overweight, and 16% are obese. Recent trends show a slowing increase in this prevalence. However, 5% of the nation's youth are considered severely obese, a trend that continues to increase among those aged 6 to 19 years [Ogden CL et al. JAMA 2010]. Aside from the psychological and physical issues associated with pediatric and adolescent obesity, the condition also increases the risk of problems later in life, including type 2 diabetes mellitus (T2DM), asthma, end-stage renal disease, obstructive sleep apnea, and severe ambulatory limitations [Inge TH et al. Pediatrics 2013].
THE IMPORTANCE OF EARLY INTERVENTION
A symposium was convened to discuss obesity-related comorbidities and strategies to mitigate the long-term effects of pediatric obesity. Aaron S. Kelly, PhD, University of Minnesota, Minneapolis, Minnesota, USA, reviewed the classifications of obesity by body mass index (BMI), the comorbidities of pediatric obesity, and the importance of early intervention.
Based on BMI percentiles, adjusted for age- and sex-specific cutoffs, the weight categories for youth are normal weight (< 85th percentile), overweight (≥ 85th to < 95th percentile), obese (≥ 95th percentile), and severe obesity (≥ 1.2 times the 95th percentile or ≥ 35 kg/m2).
Obesity affects oxidative stress and inflammation, which are associated with the development of insulin resistance and coronary heart disease. Data suggest that overweight, obese, and severely obese children have significantly higher levels of circulating oxidized low-density lipoprotein and C-reactive protein compared with normal weight children (p< .0001 for both) [Norris AL et al. Obesity (Silver Spring) 2011]. Oxidative stress and inflammation increase endothelial dysfunction, the number of circulating endothelial cells, and arterial stiffness. Targeting these pathways within the context of obesity may prevent diabetes and CHD.
Children with severe obesity have high rates (≥ 25%) of impaired glucose tolerance, an intermediate stage in the natural history of T2DM [Sinha R et al. N Engl J Med 2002], and they are 3 times more likely to have the metabolic syndrome phenotype compared with children with moderate obesity [Calcaterra V et al. Clin Endocrinol (Oxf) 2008].
Early intervention is imperative to reduce the risk of diabetes in young people, as long-term cumulative exposure to obesity and its comorbidities will likely lead to poor outcomes. The pathophysiology of diabetes and cardiovascular disease begins early in life, with obesity as a common denominator. Notably, adults who were obese as children but not as adults appear to be as healthy as their adult peers who were never obese [Juonala M et al. N Engl J Med 2011]. However, Dr. Kelly emphasized that many obese youth require treatments more intense than simply diet and exercise to address risk factors and comorbidities.
PHARMACOLOGIC THERAPY OF PEDIATRIC OBESITY
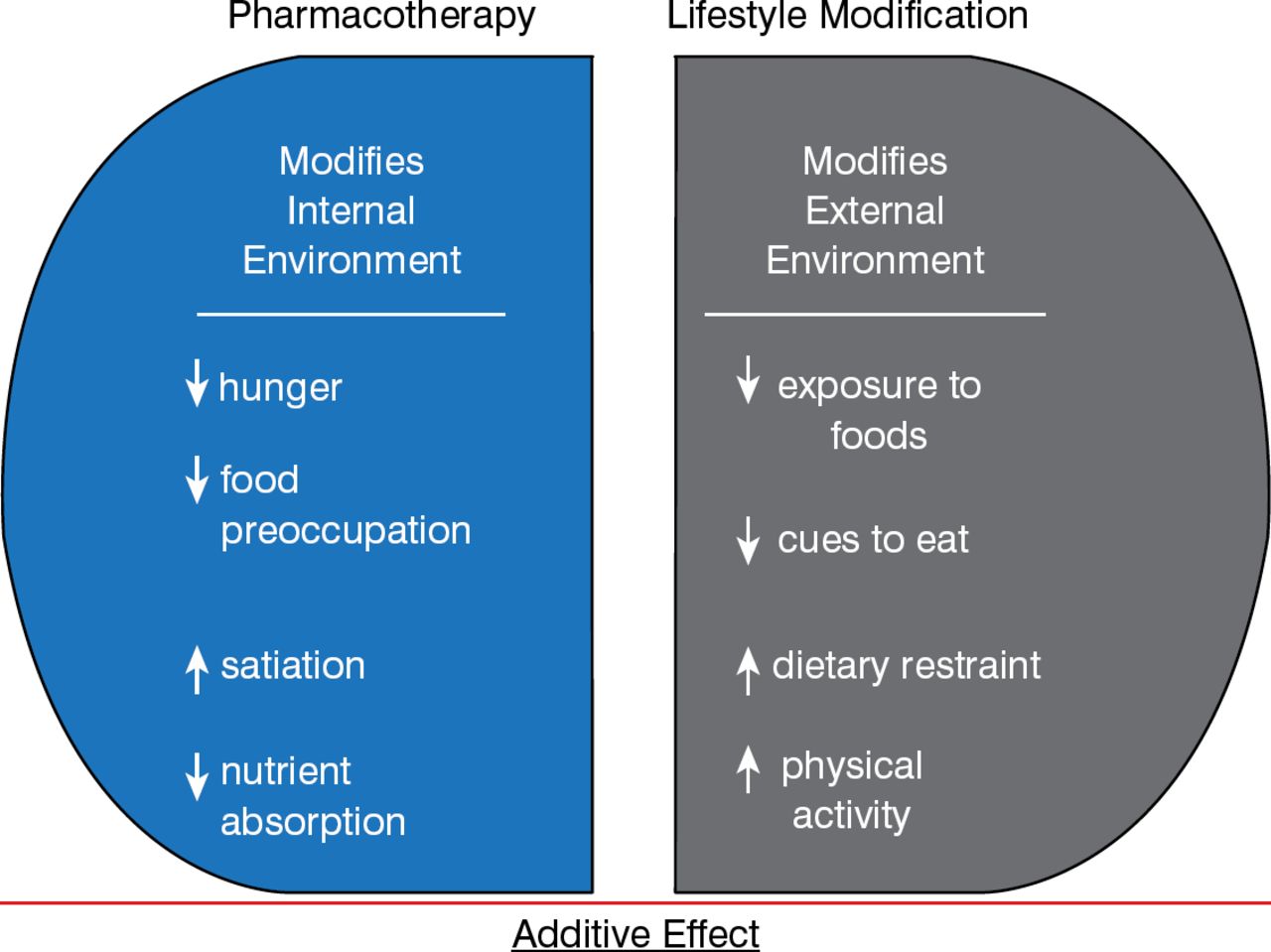
There is a paucity of data regarding the long-term pharmacologic treatment of pediatric obesity, according to Lorraine Levitt Katz, MD, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA. However, some general corollaries can be applied to both adults and children. First, pharmacotherapy may be of greater benefit for maintenance, rather than induction, of weight loss. Second, weight loss medications should be considered chronic. Third, medication should be recommended as an adjunct to diet and exercise counseling.
Lifestyle modification and pharmacotherapy augment each other and should be undertaken together (Figure 1) [Phelan S, Wadden TA. Obes Res 2002; Wadden TA et al. Arch InternMed 2001].

Benefits of Combined Treatment
Adapted from Wadden TA et al. Arch Intern Med 2001.
The only Food and Drug Administration—approved medications for long-term weight management are orlistat, lorcaserin, and a combination of phentermine and topiramate. Orlistat is the only one approved for age > 12 years. Orlistat inhibits lipases and blocks systemic absorption of dietary fat. In an adolescent obesity trial of orlistat plus lifestyle management versus placebo, significant weight loss was found (p< .001) [Chanoine JP et al. JAMA 2005]. No major safety issues were noted other than the presence of gastrointestinal (GI) symptoms in the treatment group.
Lorcaserin is approved for adults only and selectively targets the 5-HT2C receptor to increase satiety. The pivotal BLOOM trial suggested that significantly more patients on lorcaserin were able to lose ≥ 5% and ≥ 10% of their body weight at 1 year compared with placebo (p< .001 for both); a lifestyle component was recommended for all patients [Smith SR et al. N Engl J Med 2010]. Although not noted in this trial, there are ongoing safety concerns regarding cardiac valvulopathy, as well as increased risk of psychiatric, cognitive, and serotonergic adverse effects.
Controlled-release phentermine plus topiramate is approved for adults only and works by blunting appetite and prolonging satiety. After 1 year of treatment with phentermine plus topiramate, a greater proportion of the patients achieved ≥ 5% and ≥ 10% weight loss compared with placebo (p< .0001) [Allison DB et al. Obesity (Silver Spring) 2012]. Again, there are ongoing safety concerns regarding teratogenicity and increased heart rate.
SURGICAL OPTIONS
Poor health outcomes are expected in the long term as the duration of pediatric obesity takes its toll, making surgical therapy an attractive option for some younger people. Thomas Inge, MD, PhD, University of Cincinnati, Cincinnati, Ohio, USA, reinforced the fact that consideration for bariatric surgery is generally warranted only after adolescents fail other weight loss attempts and meet certain clinical, psychological, and anthropometric criteria.
The bariatric surgical approaches typically performed in adolescents include the Roux-en-Y gastric bypass (RYGB) and vertical sleeve gastrectomy (VSG). Advantages of the RYGB approach include a long history in adults, major and sustained weight loss, and reversal or improvement in comorbidities. Disadvantages include potential early complications, such as sepsis, bleeding, deep vein thrombosis or pulmonary embolus, and internal hernia. Patients are likely to develop micronutrient deficiencies. VSG is technically easier, it does not require GI anastomosis, there are no mesenteric defects, the GI tract is accessible to endoscopy, vitamin and mineral absorption is not altered, and it is possible to convert to another approach.
Data from small studies of adolescents who underwent VSG reveal that over a follow-up of 12 to 24 months, there was a 32% to 35% change in BMI [Alqahtani AR et al. Ann Surg 2012; Boza C et al. Surg Obes Relat Dis 2012]. Among 3 studies of young people who underwent RYGB, the surgery resulted in a 33% to 37% change in BMI over 1 to 2 years [Olbers T et al. Int J Obes (Lond) 2012; Inge TH et al. J Pediatr 2010; de la Cruz-Munoz N et al. Surg Obes Relat Dis 2010].
In closing, Dr. Inge emphasized that while surgical therapy in adolescents can dramatically reduce BMI and the comorbidities of obesity and improve quality of life, there are some expected adverse consequences. These include early complications, later nutrient deficiencies, and the need for health care providers who will care for and monitor these younger patients as they transition to adult primary care. Ongoing clinical research is needed to improve practice and tailor operative therapy.
Article Notes
-
↵* On September 4, 2014, the article author was changed from Mary Mosley to Jill Shuman.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.