

Summary
Over the past 20 years, the rate of obesity or overweightedness (>95th percentile for age and gender) has doubled among children and tripled among adolescents, affecting more than 5 million of them in the United States alone [O'Brien PE et al. JAMA 2010]. To date, there are no medical therapies that provide significant and durable weight loss [Barnett SJ. Curr Opin Pediatr 2011].
- Pediatric Nutrition
- Obesity
Over the past 20 years, the rate of obesity or overweightedness (>95th percentile for age and gender) has doubled among children and tripled among adolescents, affecting more than 5 million of them in the United States alone [O'Brien PE et al. JAMA 2010]. This increase has been accompanied by a dramatic rise is obesity-related health complications, including illnesses that threaten life expectancy in the absence of significant weight loss [Sarwer DB, Dilks RJ. J Youth Adolescence 2011]. To date, there are no medical therapies that provide significant and durable weight loss [Barnett SJ. Curr Opin Pediatr 2011].
Paul O'Brien, MD, Monash University, Melbourne, Australia, discussed weight loss surgery in the pediatric population. The central question that he addressed was: “Is it time?” His answer was a definitive yes. In fact, he believes it is overdue.
Prof. O'Brien discussed the variety of procedures that are available—including the laparoscopic adjustable gastric band, sleeve gastrectomy, Roux-en-Y gastric bypass (RYGB), and biliopancreatic diversion with duodenal switch. Based on invasiveness, risk, complexity, and problems, he rated them on a scale of 1 to 10, with gastric banding a 5.0 (Table 1; Figure 1).
Hierarchy of Weight Loss Techniques.

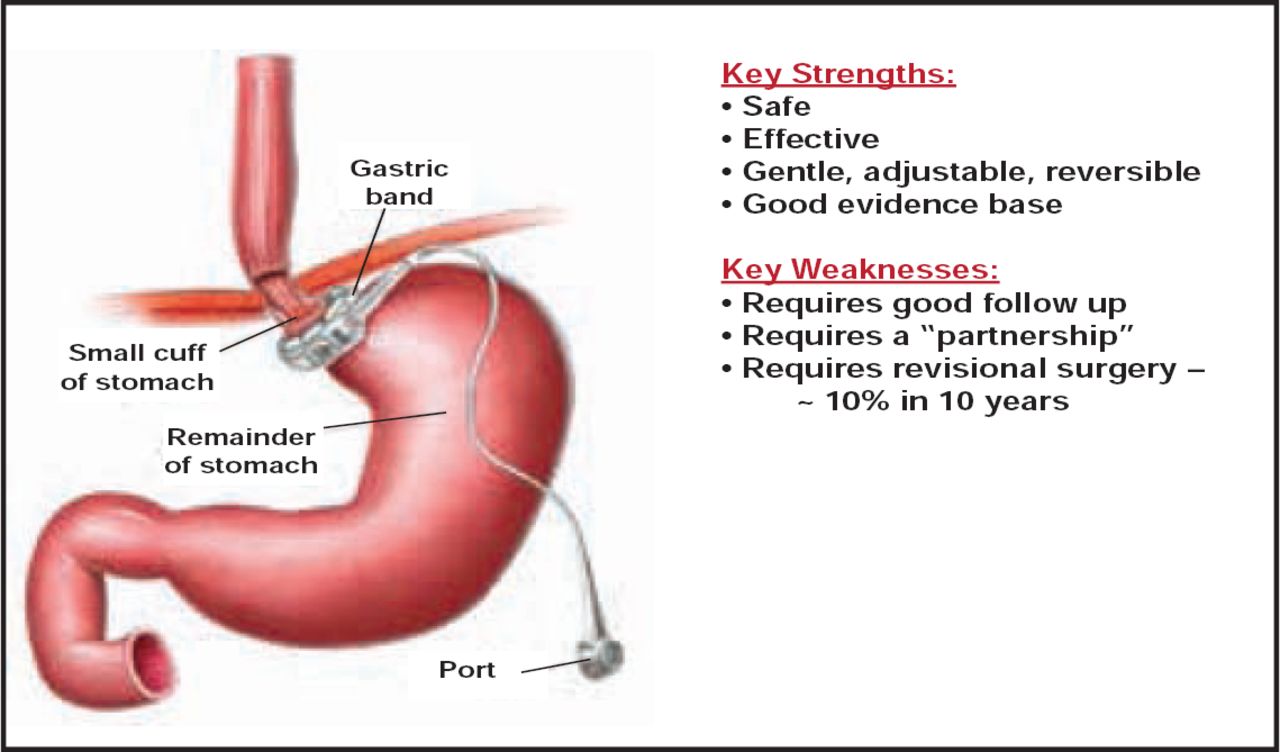
Laparoscopic Adjustable Gastric Band.
Reproduced with permission from P. O'Brien, MD.
According to Prof. O'Brien, the gastric band increases satiety and is a safe, effective, gentle, and cost-effective option that improves quality of life. In a recent study that compared the gastric band with an optimal lifestyle intervention, he and his colleagues found that 84% of obese adolescents in the surgery group and 12% in the lifestyle group lost >50% of excess weight, corrected for age. At entry, 36% of participants in the surgery group and 40% in the lifestyle group had metabolic syndrome. At 24 months, none of the adolescents who underwent surgery had it (p=0.008) compared with 22% in the lifestyle group (p=0.13) [O'Brien et al. JAMA 2010].
In adolescents, established type 2 diabetes is a strong indication for weight loss surgery [Xanthakos SA, Inge TH. J Pediatr 2007; Pratt JSA et al. Obesity 2009]. Observational studies suggest that surgically induced weight loss may be an effective treatment for the disease.
An unblended, randomized, controlled trial in adults [Dixon JB et al. JAMA 2008] found that 73% of patients in the surgical group achieved remission of type 2 diabetes versus 13% in the conventional therapy group. Meta-analyses by Buchwald et al. [Am J Med 2009] and Maggard et al. [Ann Surg 2005] found similar outcomes. In adolescents, O'Brien et al. [JAMA 2010] found that homeostasis model assessment–insulin resistance in the surgical group fell significantly from 2.94 to 0.95 after gastric banding versus 3.17 to 1.8 in the nonsurgical group.
Prof. O'Brien cited Centers of Research Excellence (CORE) criteria for pediatric weight loss surgery. They include age >14 years; body mass index >35 kg/m2 (almost always above the 99th percentile); at or near full skeletal and developmental maturity; failure in conventional programs; and an ability to understand the process and partner with the treatment team.
He noted the need to follow the CORE indications, put together a knowledgeable and caring treatment team, make sure the kids know the rules, and collect data to measure the outcomes and learn.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.