

Summary
Digital tomosynthesis (DTS) imaging is a relatively new technique that is increasingly being used for a variety of thoracic indications. This article discusses the results of the GE Healthcare VolumeRAD Lung Nodule Detection Study [NCT00963651], an international, multicenter clinical trial showing that DTS has improved sensitivity for the detection of pulmonary nodules compared with conventional conventional chest x-ray with no loss of specificity and at a similar, minimal radiation level.
- radiology clinical trials
- tomography
Digital tomosynthesis (DTS) imaging is a relatively new technique that is increasingly being used for a variety of thoracic indications. It is important that clinicians understand both the diagnostic capability of this technique and the patient dose relative to conventional chest x-ray (CXR) and computed tomography (CT). John M. Sabol, PhD, General Electric Healthcare, Waukesha, Wisconsin, USA, presented the results of the GE Healthcare VolumeRAD Lung Nodule Detection Study [NCT00963651], an international, multicenter clinical trial showing that DTS has improved sensitivity for the detection of pulmonary nodules compared with conventional CXR with no loss of specificity and at a similar, minimal radiation level (< 0.1 mSv).
The study included 158 patients (with nodules, n = 115; without nodules, n = 43) referred for diagnostic CT as part of standard of care for suspicion of pulmonary nodules or other indications. All patients received a diagnostic chest CT scan, followed by conventional posterior-anterior (PA) and lateral (LAT) CXR and then DTS. The primary objective of the study was to determine whether adding DTS to CXR increases physician accuracy in the detection of lung nodules between 3 and 20 mm in diameter when compared to conventional PA/LAT CXR. A secondary analysis was conducted to determine the relative ability of DTS plus CXR to identify nodules 3 to 4 mm, > 4 to 6 mm, > 6 to 8 mm, and > 8 to 20 mm in diameter. Other outcomes included the degree of agreement with CT for case management as defined by the Fleischner Society guidelines [MacMahon H et al. Radiology. 2005].
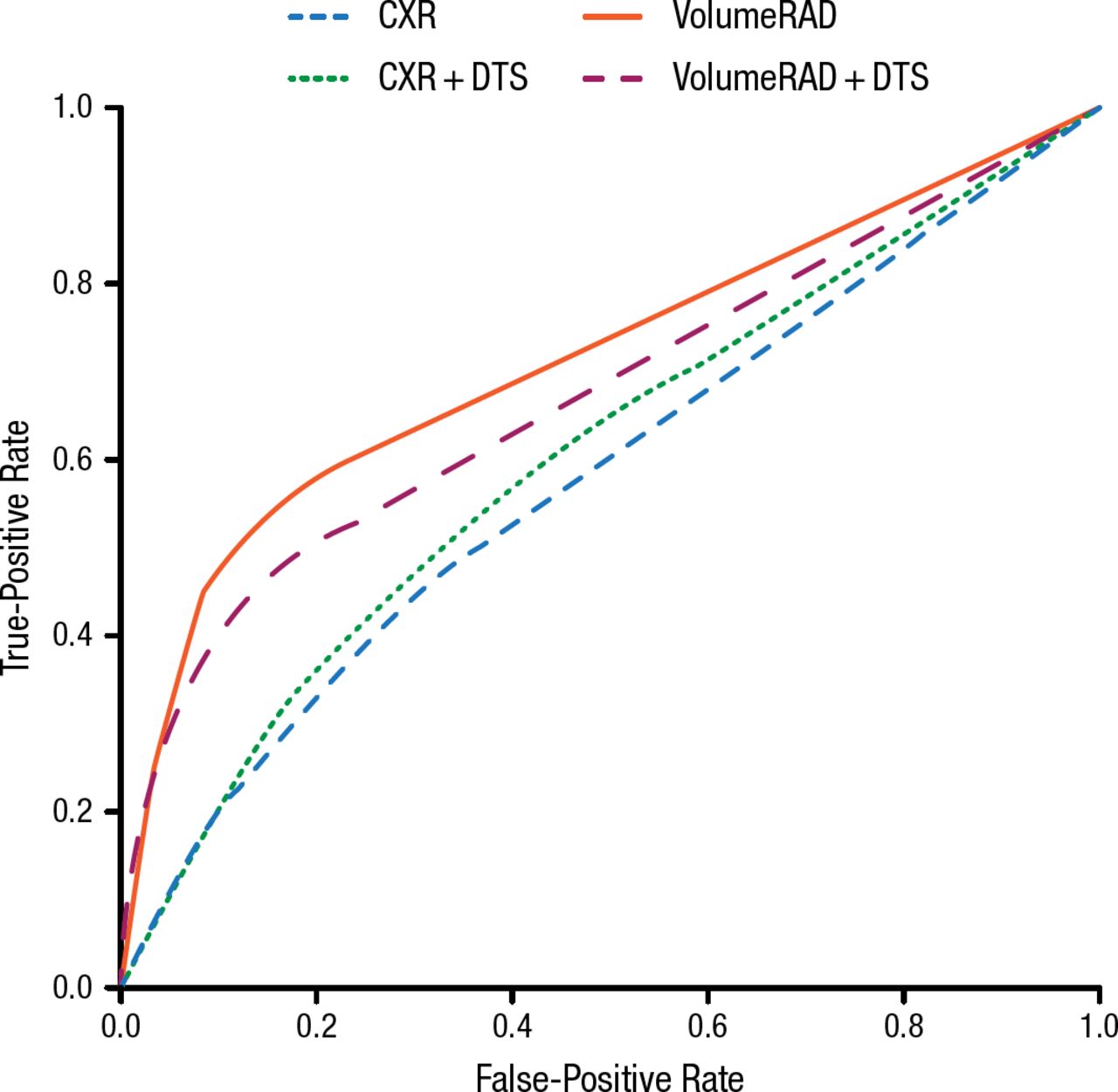
DTS was associated with a 3.6-fold improvement in sensitivity for nodules of 3 to 20 mm diameter compared with CXR. For nodules of 4 to 6 mm diameter, for which x-ray is particularly challenged, DTS showed a 7.6-fold improved sensitivity. As measured by the area under the receiver operating characteristic (ROC) curve, there was a significant increase in case management utility with tomosynthesis (Figure 1). For all nodule sizes, increases in sensitivity and area under the ROC curve were achieved with no decrease in specificity.

Case Management (Further Imaging) ROC
Tomosynthesis requires (P < .01) a smaller dose than CT and the samea (P < .01) minimal relative radiation level (< 0.1 mSv) as 2-view CXR.
ACR, American College of Radiology; CT, computed tomography; CXR, chest x-ray; DTS, digital tomosynthesis; ROC, receiver operating characteristic; VolumeRAD, GE VolumeRAD tomosynthesis.
aACR Appropriateness Criteria® Radiation Dose Assessment Introduction, 2012.
Reproduced with permission from JM Sabol, PhD.
For the effective dose calculations, digital imaging and communications in medical metadata were extracted for all image data. CT dose index and the dose-length product were calculated using the methods described in the appropriate technical reference manual. The effective dose was calculated using dose-length product conversion factors from the International Commission on Radiological Protection Publication 103 [ICRP, 2007. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37 (2–4)]. The effective dose for CXR and DTS was calculated using the PCXMC 2.0 Monte Carlo tool [Sabol JM. Med Phys. 2009]. Calculation of absorbed dose was based on estimates of incident air kerma from exposure technique data and the assumption of average-habitus patients. Data for dose estimation were available for all 158 patients in the study for some modalities and for 91 patients for all modalities. For the 91 cases with valid data for all modalities, the mean effective dose was 0.059, 0.088, and 4.86 mSv for CXR, DTS, and CT, respectively.
The effective dose of DTS was 1.5 times greater than that for 2-view CXR. The CXR and DTS effective doses were significantly less than that for CT (P < .01), and the same minimal relative radiation level (< 0.1 mSv) as that of 2-view CXR.
To conclude, DTS is a low-dose option for volumetric thoracic imaging and improves lung nodule detection.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.