

Summary
Mammograms are said to detect 80% to 85% of all breast cancers. Women with densities in at least 65% of their breasts are estimated to have a 4- to 6-fold increased risk of breast cancer when compared to women with less dense breasts. Innovations in magnetic resonance imaging (MRI) and computer technology have led to improved scanning strategies, transmission characteristics, and image resolution, as discussed in this article.
- magnetic resonance imaging
- breast cancer
Mammograms are said to detect 80% to 85% of all breast cancers. According to speaker David A. Strahle, MD, Regional Medical Imaging, Flint, Michigan, USA, mammograms “eventually” pick up 80% to 85% of all breast cancers, after accounting for women with dense breasts, whose cancers are often missed on the initial and often subsequent mammograms—a delay that could change the course of the disease. Women with densities in at least 65% of their breasts are estimated to have a 4- to 6-fold increased risk of breast cancer when compared to women with less dense breasts [Ginsburg OM et al. Br J Cancer. 2008]. Approximately one-half to three-quarters of all women in their 40s and 50s may have a breast density ≥ 50% [Checka CM et al. AJR Am J Roentgenol. 2012].
Innovations in magnetic resonance imaging (MRI) and computer technology have led to improved scanning strategies, transmission characteristics, and image resolution. As tumors grow, they develop a neovascular network necessary for invasion and metastasis. Once a tumor develops these abnormal vessels, it becomes detectable by MRI down to about 3 mm.
Dr Strahle and his team designed a protocol to evaluate the role that dense fibroglandular tissue (FGT) plays in obscuring breast cancer, and they explored the feasibility of using a limited number of MRI sequences for a national screening program. From 2009 to 2011, 671 random average-risk women with negative screening mammograms were offered free breast-screening MRI. Seventeen parameters were recorded, including percentage volume of FGT, brightness of the FGT density, and location of any lesions inside or outside of FGT. Simplified reading criteria were developed to standardize interpretation so that an average MRI reader in clinical practice could quickly interpret the images.
In 208 of the 671 women, 315 abnormalities not seen on the screening mammogram were detected with MRI. Of these, 7 masses were identified as malignant by MRI and confirmed on biopsy as 1 invasive lobular carcinoma, 3 invasive ductal carcinomas, and 3 ductal carcinoma in situ (DCIS) lesions. All of the cancers were hidden within FGT occupying ≥ 50% of the breast volume. All of the cancers were detected with only 2 MRI sequences (4 acquisitions), requiring only 7.5 minutes of scan time. According to Dr Strahle, this rapid MRI screening protocol reduced the MRI cost by > 50%.
Rapid MRI had a 57% false-positive biopsy rate, with a reduction of 50% in the number of biopsies and a positive predictive value of 41%. Additionally, 364 of the mammographic Breast Imaging Reporting and Data System (BI-RADS) codes were changed, as one-half of the recorded mammographic BI-RADS codes were in error.
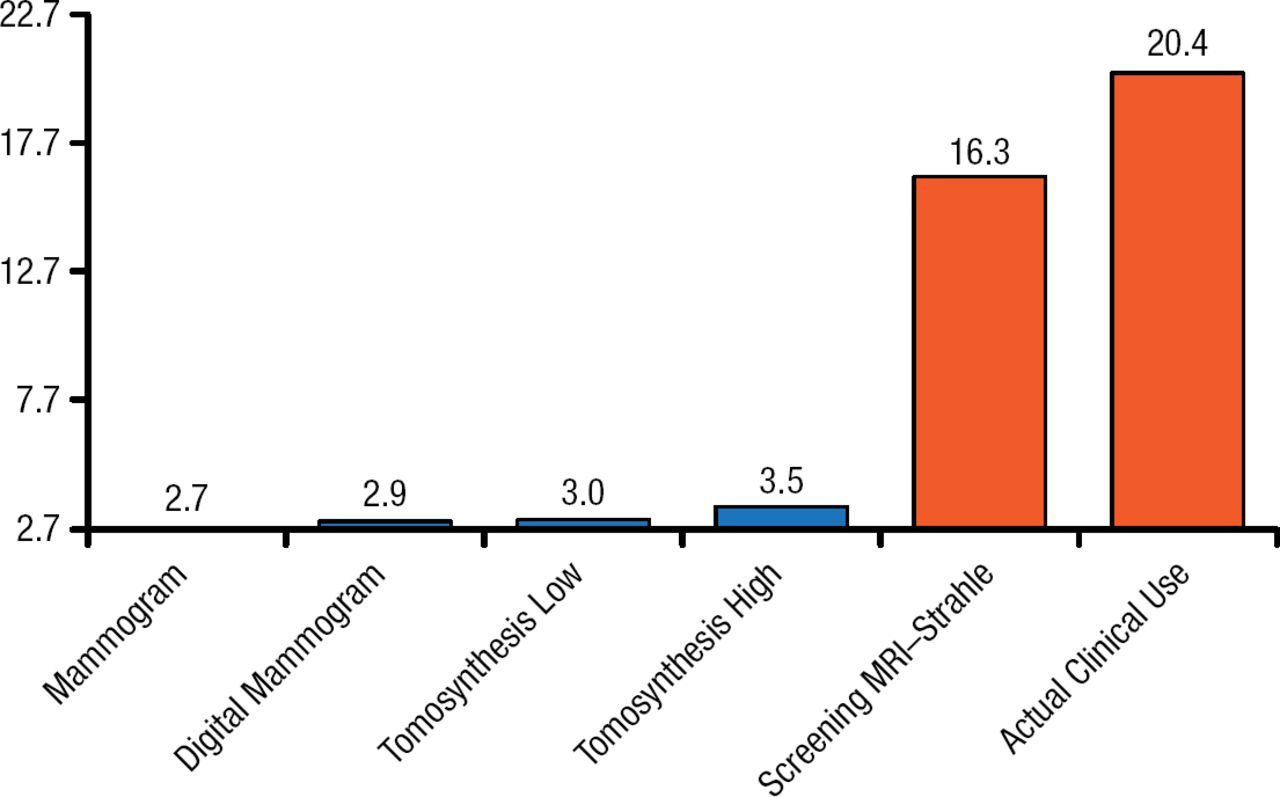
Current data suggest that screening mammograms detect 2.7 cancers per 1000 women per year in the general population [Arleo EK et al. AHR Am J Roentgenol. 2013]. By adding MRI to the mammogram in women with ≥ 50% FGT, Dr Strahle and his group detected additional cancers at a rate of 16.3 per 1000 women per year. With a screening-mammogram detection rate of 2.7, it could take up to 6 years to eventually identify all 16.3 cancers found on MRI.
He then went on to speak about microcalcifications of the breast, which occasionally develop in the presence of a few small, slow-growing cancers and are often picked up on a mammogram. Many of these microcalcifications are not visible on MRI, because they have not yet developed the neovasculature needed for identification by MRI. For this reason, the American College of Radiology guidelines have determined that mammography is the most appropriate radiologic procedure for women with breast microcalcifications [Comstock CH et al. National Guideline Clearinghouse. 2009].
Because DCIS is characterized by microcalcifications in the affected milk ducts, conventional wisdom has held that MRI was unsuited for detecting this early stage of breast cancer. However, data suggest that the sensitivity of MRI for detecting DCIS is actually much higher than that of mammography [Kuhl CK et al. Lancet. 2007]. This may be due to the fact that fast-growing DCIS lesions do not always develop microcalcifications. Instead, high-grade DCIS appears to be pervaded by many small blood vessels that are clearly visible on MRI.
Currently, breast MRI is used only after a mammogram has initially detected an abnormality, which, according to Dr Strahle, “severely limits MRI's ability to change the course of the disease.” He believes that after identification of tumors both small and large during the first year of a national MRI screening program, subsequent years of screening will result in identification of smaller and smaller tumors, further reducing the need for chemotherapy and radiotherapy.
In September 2012, Dr Strahle's practice began using the rapid MRI protocol for women with dense breasts. In the last 2 years, 1 cancer has been found for every 344 women screened by mammography and 1 cancer for every 60 women screened by MRI. A comparison of reimbursement in the practice found that the additional cost of screening MRI per woman was US$72, adding only a 28% increase to the total mammography budget. Screening MRI helps to avoid the costs associated with late identification and treatment. According to Dr Strahle, the total dollar savings are high enough to absorb the cost of both mammograms and MRI while yielding a significant net savings. Based on these data, at least 1 insurance carrier in Michigan has agreed to reimburse for routine breast-screening MRI using the rapid protocol.
Currently, breast tomosynthesis and automated 3D breast ultrasound are being marketed at substantially increased cost, but both may require added mammogram views and unnecessary biopsies as well. Figure 1 compares the detection rates of several screening technologies.

Breast Cancer Detection Rate per 1000 Women
MRI, magnetic resonance imaging.
Reproduced with permission from DA Strahle, MD.
Dr Strahle concluded that while mammography should remain the standard of care for women with < 50% FGT, MRI should be used in place of, or in addition to, mammography for screening women with dense breasts > 50% FGT. He estimates that with 35% unused capacity in radiology facilities throughout the United States, at least two-thirds of women with dense breasts could undergo MRI scanning without additional facility costs or the purchase of any new technology.

The editors would like to thank the many members of the Radiological Society of North America 100th Scientific Assembly and Annual Meeting presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2015 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.