

Summary
The characteristics, benefits, and uses of a number of new technologies in cardiac electrophysiology (EP) technologies were reviewed. These technologies and devices included 3D mapping technologies, high-density MRI-guided mapping, focal impulse and rotor modulation, body surface mapping, and a left atrial appendage closure device called the Watchman.
- arrhythmias
- cardiac electrophysiology
- atrial fibrillation
- catheter ablation
- cerebrovascular disease
- cardiology & cardiovascular medicine clinical trials
Mohammad Shenasa, MD, PhD, O'Connor Hospital, San Jose, California, USA, reviewed a few of the new cardiac electrophysiology technologies that are being used in clinical practice.
Three-dimensional mapping technologies, used to facilitate spatial orientation within complex cardiac anatomies, are now being integrated with conventional fluoroscopy imaging. With the use of prerecorded fluoroscopy cine-loops, stored real-time catheter location data can be visualized nonfluoroscopically within a radiographic environment. The speed of the cine-loop is matched to the real-time electrocardiogram signal. Atrial fibrillation (AF) ablation based on this technology reduces radiation exposure and may have a lower complication rate when compared to ablation based on conventional technology [Sommer P et al. Circ Arrhythm Electrophysiol. 2014].
Another new technology, high-density magnetic resonance imaging (MRI)–guided mapping, is particularly useful for mapping sinus node activation. Ablation with MRI-guided mapping has already been done at several institutions and appears safe. MRI interventional suites for mapping and ablation are now available for the specific use of this technique [Eitel C et al. Eur Heart J. 2012; Piorkowski C et al. Circ Arrhythm Electrophysiol. 2013].
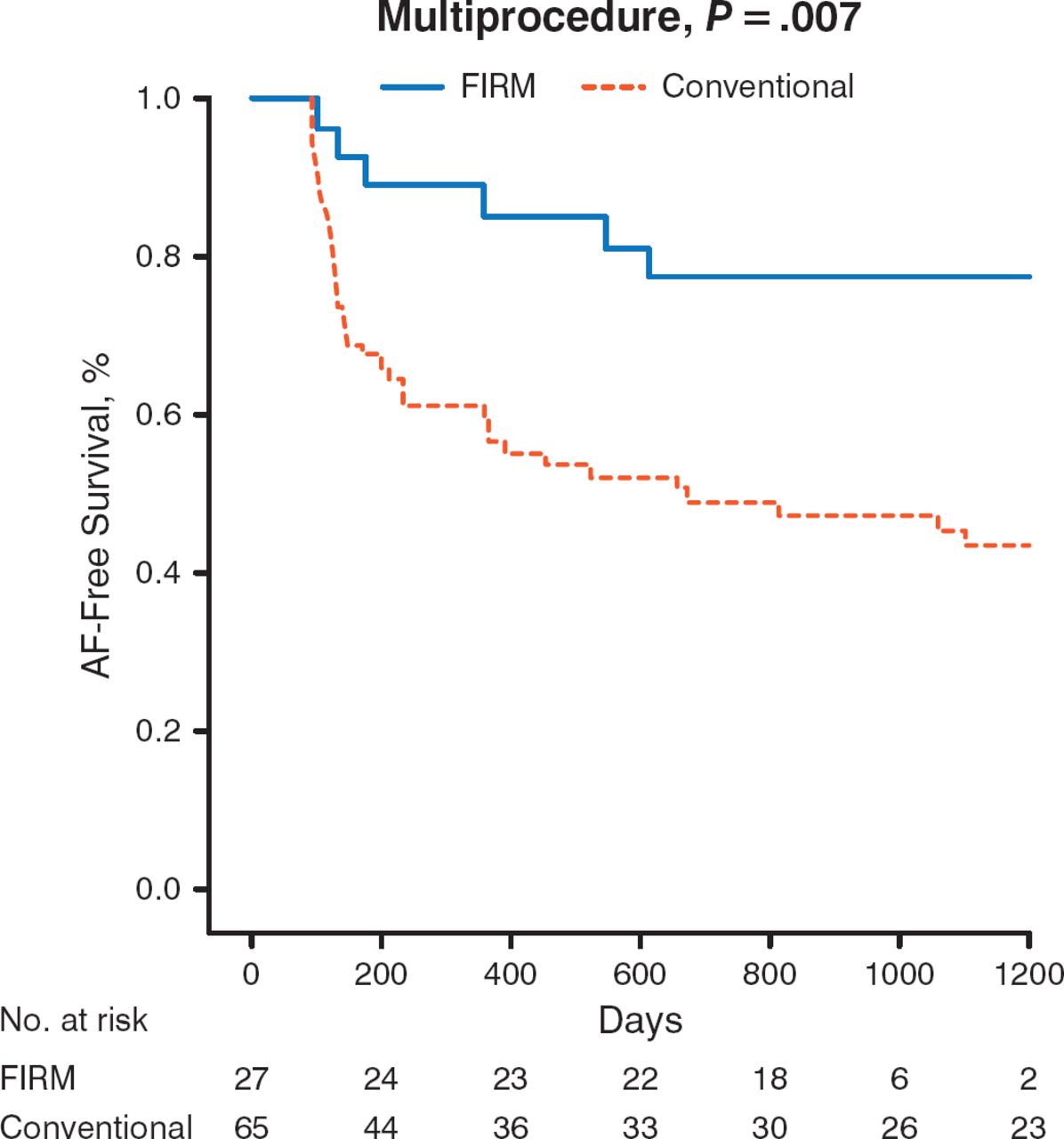
Elimination of patient-specific localized sources of AF by focal impulse and rotor modulation (FIRM) ablation can also terminate or slow the AF while improving outcomes. For instance, FIRM at the inferior left atrial rotor terminates AF to sinus in < 1 minute [Narayan SM et al. J Am Coll Cardiol. 2012]. FIRM ablation promotes freedom from AF for up to 3 years when compared with conventional ablation (Figure 1) [Narayan SM et al. J Am Coll Cardiol. 2014].

Freedom From AF
AF, atrial fibrillation; FIRM, focal impulse and rotor modulation.
Adapted from the Journal of the American College of Cardiology, 63, Narayan SM et al, Ablation of Rotor and Focal Sources Reduces Late Recurrence of Atrial Fibrillation Compared With Trigger Ablation Alone: Extended Follow-up of the CONFIRM Trial (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation), 1761–1768, Copyright (2014), with permission from American College of Cardiology Foundation.
Body surface mapping provides accurate maps of localized arrhythmias, which may shorten procedural time [Haissaguerre M et al. J Cardiovasc Electrophysiol. 2013]. For patients with AF, it allows unprecedented 3D vision of individual clusters of AF drivers, allowing a high rate of AF termination with significantly less radiofrequency delivery. Additional studies are evaluating ways to improve signaling in damaged tissue and integrate other imaging modalities (eg, MRI).
New and smaller pacemakers are being developed as well. The leadless pacer, < 10% of the size of a conventional pacemaker, is implanted via a catheter inside the heart. It attaches to the wall of the right ventricular apex with a screw-in active fixation mechanism. Battery longevity is comparable to conventional pacemakers, with an average life span of 8.4 years at 100% pacing. The device is fully retrievable for repositioning, if necessary.
The first-generation subcutaneous implantable cardioverter defibrillator detects and terminates induced and spontaneous ventricular fibrillation (VF) and is suitable for a broad range of indications, including ischemic and idiopathic VF and channelopathy-related ventricular tachyarrhythmias. It is also an option for candidates who do not require pacing for bradycardia, cardiac resynchronization, or antitachycardia [Crozier I et al. Card Electrophysiol Clin. 2014].
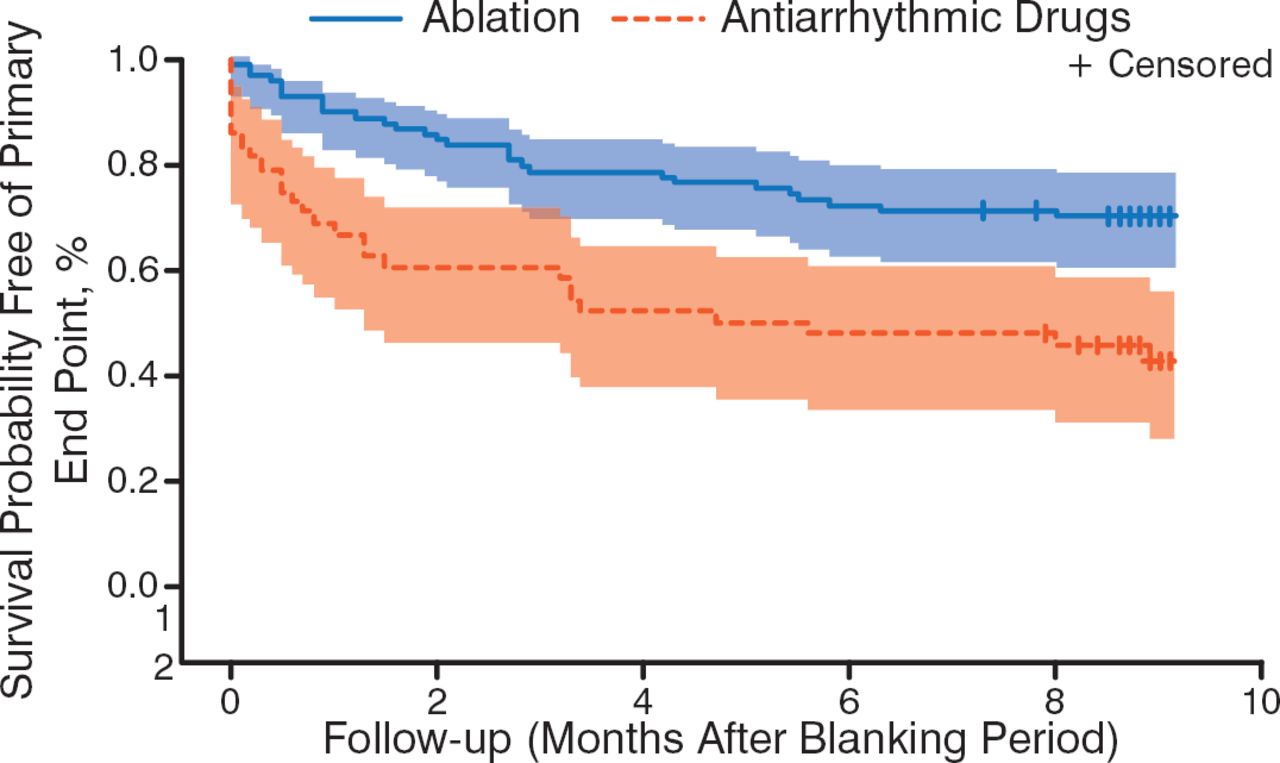
In patients with paroxysmal and persistent AF, strategies for rhythm control often include antiarrhythmic drug treatment (eg, beta-blockers, diltiazem, verapamil, amiodarone) along with catheter ablation. Studies have reported that catheter ablation is superior to antiarrhythmic drug therapy for the maintenance of sinus rhythm in patients with persistent AF (Figure 2) [Mont L et al. Eur Heart J. 2014] and paroxysmal AF [Morillo CA et al. JAMA. 2014].

Sinus Rhythm Better Maintained With Ablation Compared With Antiarrhythmic Drugs
Shading indicates standard deviation.
Adapted from Mont L et al. Catheter ablation vs. antiarrhythmic drug treatment of persistent atrial fibrillation: a multicentre, randomized, controlled trial (SARA study). Eur Heart J. 2014;35:501–507. By permission from European Society of Cardiology.
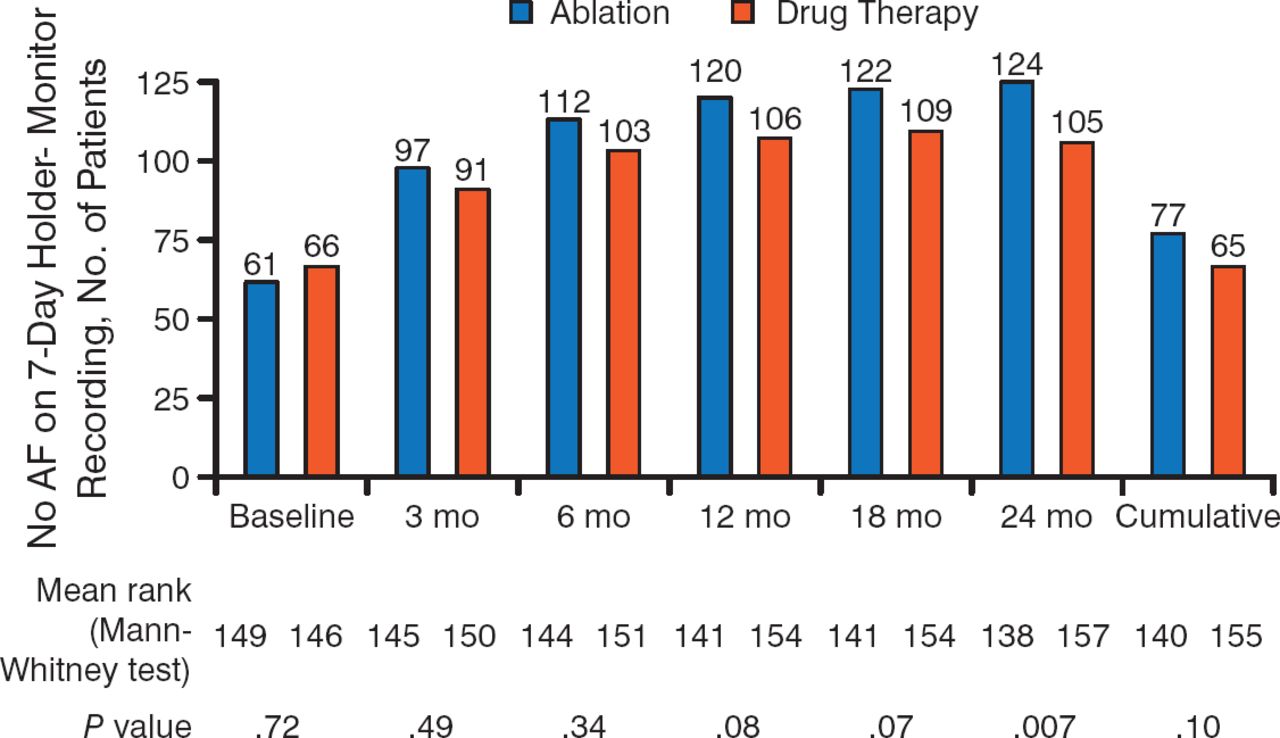
However, another study reported no significant difference (P = .10) in the cumulative burden of AF over a 2-year period when comparing radiofrequency ablation with antiarrhythmic drug therapy as a first-line treatment in patients with paroxysmal AF (Figure 3) [Cosedis Nielsen J et al. N Engl J Med. 2012]. Nevertheless, more patients in the ablation group were free from any AF (85% vs 71%; P = .004) and symptomatic AF (93% vs 84%; P = .01).

No Difference in Cumulative Burden of AF Between Ablation and Drug Therapy
AF, atrial fibrillation.
Adapted from N Engl J Med. Cosedis Nielsen J et al, Radiofrequency Ablation as Initial Therapy in Paroxysmal Atrial Fibrillation, 367, 1587–1595. Copyright © (2012) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
In patients with mild heart failure, left ventricular dysfunction, and left bundle branch block, early intervention with cardiac resynchronization therapy and a defibrillator is associated with significant long-term survival (7 years). This benefit was not seen in patients without left bundle branch block [Goldenberg I et al. N Engl J Med. 2014].
The final technology that Prof Shenasa discussed was the Watchman, a left atrial appendage closure device that was evaluated in the PROTECT AF trial [NCT00129545] and found to be noninferior to warfarin in patients with nonvalvular AF for prevention of stroke [Holmes DR et al. Lancet. 2009]. In a subsequent analysis, the Watchman was associated with a significant improvement in quality of life on the Short-Form 12 Health Survey for total physical score, physical function, and physical role limitation as compared with the warfarin-treated patients [Alli O et al. J Am Coll Cardiol. 2013].
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.