

Summary
According to a report from the Centers for Disease Control and Prevention (CDC), overweight or obese preschoolers are five times as likely to become overweight or obese adults as their normal weight peers [Centers for Disease Control and Prevention. Morb Mortal Wkly Rep 2013]. Additionally, high cholesterol, high blood sugar, asthma, and mental health problems are linked to obesity in older children and adolescents. American society is characterized by environments that promote poor eating habits and physical inactivity. This article discusses intervention strategies to address some of these issues.
- Obesity
- Pediatric Nutrition
- Exclusive Article - For home page
- Nutrition
- Obesity
- Pediatric Nutrition
According to a report from the Centers for Disease Control and Prevention (CDC), overweight or obese preschoolers are five times as likely to become overweight or obese adults as their normal weight peers [Centers for Disease Control and Prevention. Morb Mortal Wkly Rep 2013]. Additionally, high cholesterol, high blood sugar, asthma, and mental health problems are linked to obesity in older children and adolescents.
Although small decreases in the prevalence of obesity were observed among low-income preschool children in certain parts of the United States and its territories between 2008 and 2011, the rate of obesity remains high with ∼1 of 8 children aged 2 to 5 years having an age- and sex-specific body mass index (BMI) ≥95th percentile, according to the 2000 CDC growth charts (Figure 1) [Centers for Disease Control and Prevention. Morb Mortal Wkly Rep 2013]. The study included data for ∼11.6 million low-income children aged 2 to 4 years who were participants in federally funded child health and nutrition programs.

Changes in Obesity Prevalence: 2008 to 2011
DC=Washington, DC; PR=Puerto Rico; VI=Virgin Islands.
Source: Morbidity and Mortality Weekly Report 2013.
Using a subset of the CDC data, Pan and colleagues [Pediatrics 2013] reported an overall incidence of childhood obesity of 11.0% but with several important differences among population subgroups. Obesity was more common among boys versus girls and among children aged 0 to 11 months in 2008 versus older children. The risk of obesity was 35% higher among Hispanics and 49% higher among American Indians/Alaska Natives compared with non-Hispanic whites, but among non-Hispanic African Americans, it was 8% lower. Of the children who were obese at baseline, 36.5% remained obese at follow-up while 63.5% were nonobese. Obesity remission was proportionally significantly lower among Hispanics and American Indians/Alaska Natives compared with other racial/ethnic groups.
American society is characterized by environments that promote poor eating habits and physical inactivity. William H. Dietz, MD, PhD, Centers for Disease Control and Prevention, Atlanta, Georgia, USA, discussed intervention strategies to address some of these issues.
Beyond the effects of poverty, pregnancy and postnatal influences have an important influence on childhood obesity. These include maternal weight prior to pregnancy and the amount of weight gained during pregnancy, breastfeeding duration, the child's overall feeding experience and sleep patterns, as well as media exposure to food marketing strategies in older children.
Despite the fact that breastfeeding provides optimal nutrients for infant growth and development and enhances an infant's immunologic defenses, many American women opt not to breastfeed. Among the many reasons for this decision may be a mother's experience during her hospital stay. Results of a study of these experiences found that the number of “baby-friendly” steps the mother experienced in the hospital effectively predicted her breastfeeding duration [DiGirolamo AM et al. Pediatrics 2008].
How we encourage our children to eat is also important to establishing healthy eating. Some of the feeding practices that influence food consumption among young children are shown in Table 1. Among parenting styles, an authoritarian approach is associated with the highest risk of overweight among young children, while children with authoritative mothers have the lowest risk [Rhee KE et al. Pediatrics 2006].
Feeding Practices That Influence Food Consumption in Young Children
Several government programs like the Let's Move Child Care Challenge are attempting to help manage the obesity issue, but only one study has looked at the effect of these programs [Quattrin T et al. Pediatrics 2012]. The study tested the efficacy of an innovative family-based intervention for overweight preschool-aged children and overweight parents conducted in the primary care setting. After 6 months, parents and children (aged 2 to 5 years) in the intervention group had significant reductions in BMI with parent and child weight changes correlating. The lessons from this study suggest children's diets cannot be considered in the absence of parenting practices. Parental input is an important component to good infant and childhood eating habits. This information should be incorporated into existing programs and messaged across all areas dealing with childhood obesity with consistency.
When all other means of intervention have failed for weight loss, Thomas H. Inge, MD, PhD, University of Cincinnati, Cincinnati, Ohio, USA, believes bariatric surgery is a viable option for children. The use of weight-loss surgery has tripled since 2000 [Kelleher DC et al. JAMA Pediatr 2013] especially in the severely obese, who often suffer from a number of comorbid illnesses, including dyslipidemia, sleep apnea, and hypertension [Inge TH et al. Pediatrics 2014].
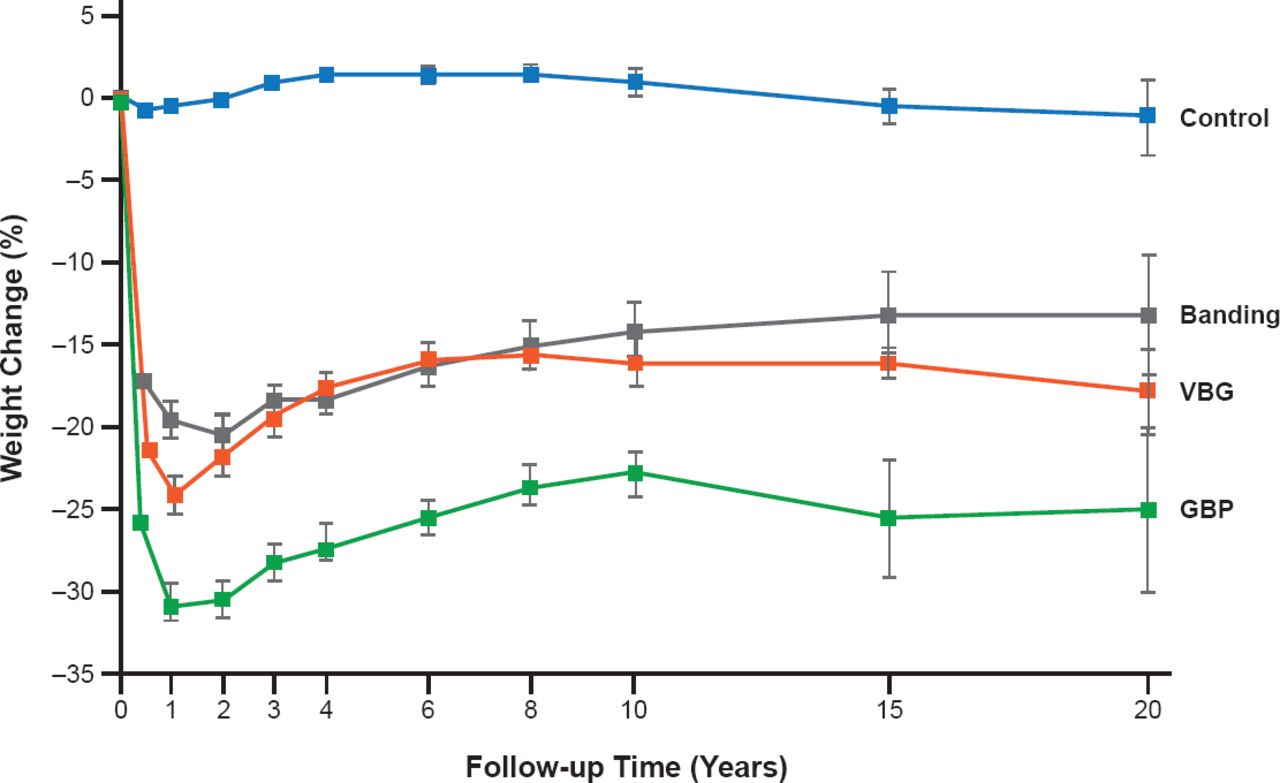
There are three main approaches to weight-loss surgery: laparoscopic Roux-en-Y gastric bypass, vertical sleeve gastrectomy, and adjustable gastric banding. The Swedish Obese Subjects (SOS) study reported significant weight loss using all three approaches (Figure 2) [Sjöström L et al. JAMA 2012].

Swedish Obese Subjects Study Results
GBP=gastric bypass; VBG=vertical-banded gastroplasty.
Reproduced from Sjöström L et al. Bariatric surgery and long-term cardiovascular events. JAMA 2012; 307(1):56–65. With permission from the American Medical Association.
Maximum weight losses in the surgical subgroups were observed after 1 to 2 years: gastric bypass, 32%; vertical-banded gastroplasty, 25%; and banding, 20% [Sjöström L et al. N Engl J Med 2007]. Weight losses from baseline stabilized at 25%, 16%, and 14%, respectively, after 10 years. The cumulative risk of mortality was significantly less in the surgery group compared with controls (p=0.01).
The Roux-en-Y gastric bypass approach is the gold standard and offers rapid and sustainable weight loss. Disadvantages include potentially serious complications and the development of common vitamin deficiencies (iron, vitamin B12, vitamin D, and thiamine). Advantages of vertical sleeve gastrectomy include technical ease, no gastrointestinal anastomosis, no mesenteric defects, GI tract accessible to endoscopy, vitamin and mineral adsorption not altered, ability to convert procedure to two other operations, no device to erode, and no adjustments needed. Lap adjustable gastric banding is a relatively quick procedure (45 to 60 minutes), with same day or next day discharge and with no stapling or cutting of the stomach or intestine, and is currently approved only for patients aged ≥18 years in the United States. There is less weight loss with the band, however.
In summary noted Dr. Inge, severe pediatric obesity is becoming more common. Weight-loss surgery offers dramatic reduction in BMI and enhanced quality of life. Caution is advised in that surgical therapy may produce early complications and later nutritional complications. Ongoing clinical research efforts will be needed to improve technique.
In a poster session, Jamie L. Pula, PhD, RD, St. Joseph's Regional Medical Center, Paterson, New Jersey, USA, presented data regarding parental perceptions regarding obese and nonobese school-aged children of predominately Hispanic and African heritage [Pula J, Lamacchia M. ASN 2013 (abstr 36)]. She reported that parents of overweight or obese females, compared with parents of overweight or obese males, are more perceptive of the impact of obesity on their child's emotions, health, and quality of life.
Dr. Pula also presented data from a school-based, prospective, case-control, before and after, interventional study in inner-city children based on the United States Department of Agriculture wellness programs MyPlate and Let's Move [www.choosemyplate.gov]. Measured outcomes included changes in the 3-minute step test and vertical jump test [Pula J, Lamacchia M. ASN 2013 (abstr 37)]. After 12 weeks, the 3-minute step test (p=0.0011) and vertical jump test (p=0.0437) scores significantly improved in the female students. In addition resting heart rate also significantly (p=0.0008) improved. Similar findings were not noted in the boys.
Dr. Pula suggested that the weight management program may have helped the female students develop stronger muscles and a more efficient cardiovascular system. Why this did not occur among the male students was not explained.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.